

Acute heart failure and iron deficiency: a prospective, multicentre, observational study
- PMID: 34862747
- PMCID: PMC8788059
- DOI: 10.1002/ehf2.13737
Acute heart failure and iron deficiency: a prospective, multicentre, observational study
Abstract
Aims: The prevalence and the natural course of iron deficiency (ID) in acute heart failure (AHF) are still unclear. We investigated the prevalence of ID in unselected patients admitted with AHF on admission, at discharge and up to 3 months thereafter.
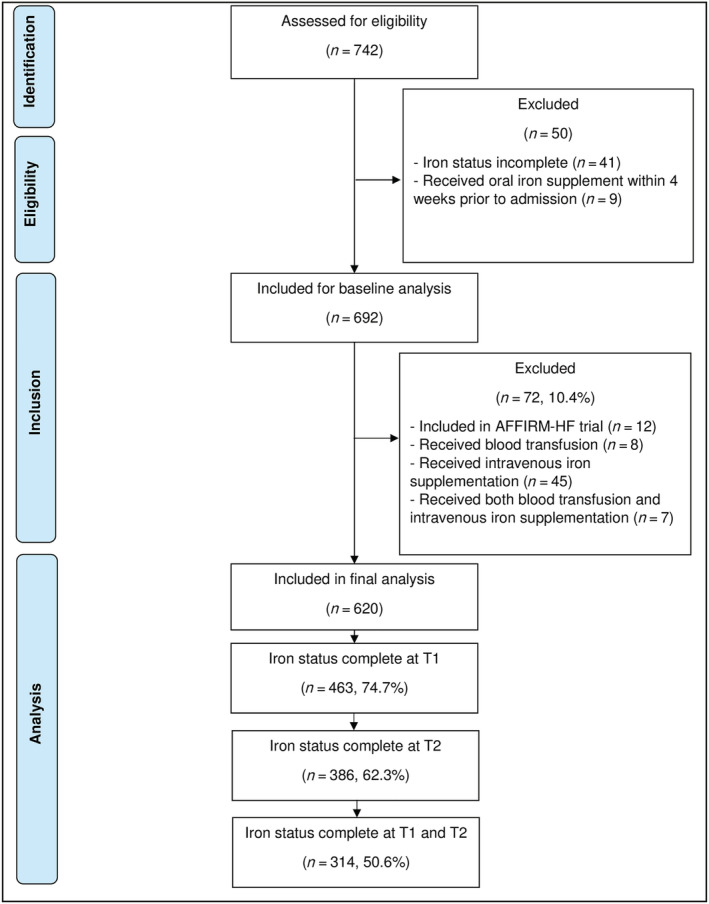
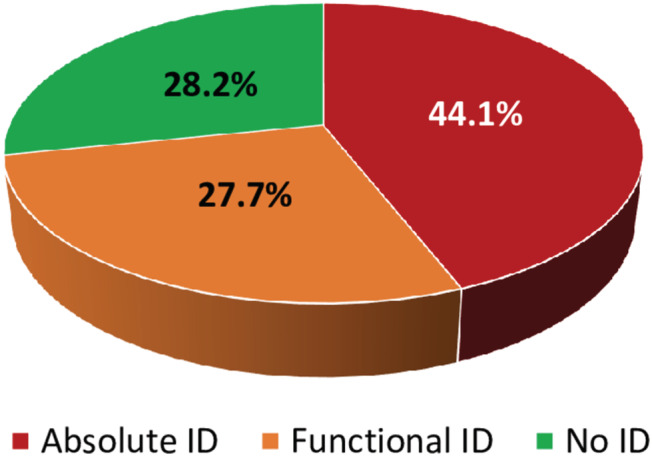
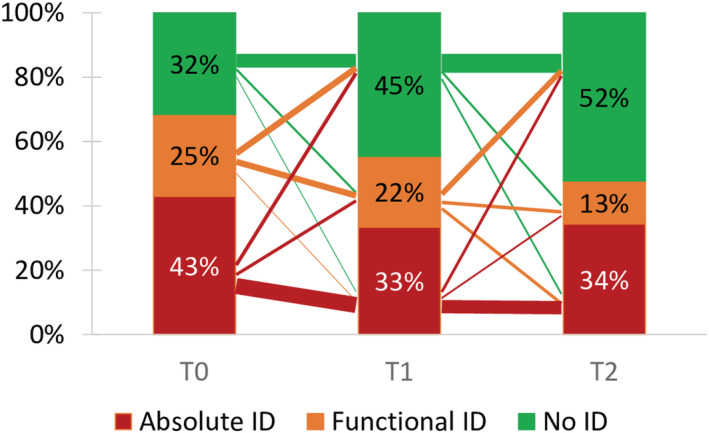
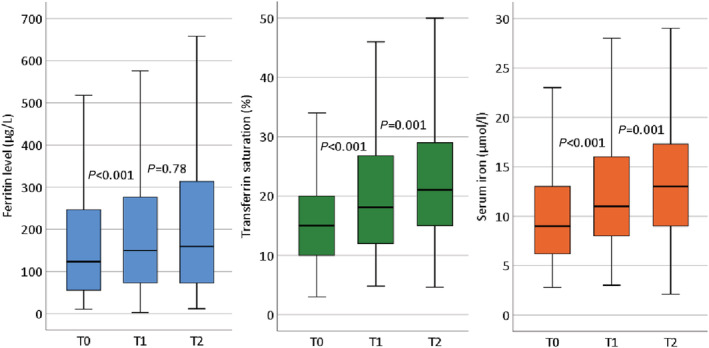
Methods and results: In this prospective, multicentre, observational study, 742 patients admitted with AHF were enrolled. The main study outcome was the percentage of patients with ID (ferritin <100 μg/L = absolute ID or ferritin 100-299 μg/L and transferrin saturation <20% = functional ID) at admission (T0), after clinical stabilization prior to discharge (T1), and 10 ± 6 weeks after discharge (T2). At T0, ID was present in 71.8% of the patients (44.1% absolute and 27.7% functional ID). At T1 and T2, ID was present in 56.4% (32.4% absolute and 24% functional ID) and 50.3% (36.8% absolute and 13.5% functional ID), respectively. Absolute ID persisted from T0 to T2 in 66% of the patients, while functional ID resolved in 56% of the patients. Ferritin (median [interquartile range] 124 μg/L [56-247] to 150 μg/L [73-277]), transferrin saturation (15% [10-20] to 18% [12-27]), and iron levels (9 μmol/L [6-13] to 11 μmol/L [8-16]) increased significantly (all P < 0.001) from T0 to T1. Transferrin saturation (to 21% [15-29]) and iron levels (to 13 μmol/L [9-17]) also increased significantly (both P < 0.01) from T1 to T2 without iron supplementation.
Conclusions: Iron deficiency is highly prevalent in patients with AHF, but resolves during treatment in some patients, even without iron supplementation. Absolute ID is more likely to persist over time, whereas functional ID often resolves during treatment of AHF, representing probably a reduced iron availability rather than a true deficiency.
Keywords: Acute decompensated heart failure; Comorbidity; Functional iron deficiency; Iron availability disorder; Iron deficiency; Worsening heart failure.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
H‐PB‐LR, CvD, and ME report receiving advisory board fees and lecture fees from Vifor Pharma. HK and CK received lecture fees from Vifor Pharma. The other authors have no conflicts of interest to declare.
Figures
References
-
- Jankowska EA, Rozentryt P, Witkowska A, Nowak J, Hartmann O, Ponikowska B, Borodulin‐Nadzieja L, Banasiak W, Polonski L, Filippatos G, McMurray JJ, Anker SD, Ponikowski P. Iron deficiency: an ominous sign in patients with systolic chronic heart failure. Eur Heart J 2010; 31: 1872–1880. - PubMed
-
- Klip IT, Comin‐Colet J, Voors AA, Ponikowski P, Enjuanes C, Banasiak W, Lok DJ, Rosentryt P, Torrens A, Polonski L, van Veldhuisen DJ, van der Meer P, Jankowska EA. Iron deficiency in chronic heart failure: an international pooled analysis. Am Heart J 2013; 165: 575–582.e3. - PubMed
-
- Cohen‐Solal A, Damy T, Terbah M, Kerebel S, Baguet JP, Hanon O, Zannad F, Laperche T, Leclercq C, Concas V, Duvillié L, Darné B, Anker S, Mebazaa A. High prevalence of iron deficiency in patients with acute decompensated heart failure. Eur J Heart Fail 2014; 16: 984–991. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
