

The severity of neuropsychiatric symptoms is higher in early-onset than late-onset Alzheimer's disease
- PMID: 34862834
- PMCID: PMC8901553
- DOI: 10.1111/ene.15203
The severity of neuropsychiatric symptoms is higher in early-onset than late-onset Alzheimer's disease
Abstract
Background and purpose: The faster rates of cognitive decline and predominance of atypical forms in early-onset Alzheimer's disease (EOAD) suggest that neuropsychiatric symptoms could be different in EOAD compared to late-onset AD (LOAD); however, prior studies based on non-biomarker-diagnosed cohorts show discordant results. Our goal was to determine the profile of neuropsychiatric symptoms in EOAD and LOAD, in a cohort with biomarker/postmortem-confirmed diagnoses. Additionally, the contribution of co-pathologies was explored.
Methods: In all, 219 participants (135 EOAD, 84 LOAD) meeting National Institute on Aging and Alzheimer's Association criteria for AD (115 amyloid positron emission tomography/cerebrospinal fluid biomarkers, 104 postmortem diagnosis) at the University of California San Francisco were evaluated. The Neuropsychiatric Inventory-Questionnaire (NPI-Q) was assessed at baseline and during follow-up. The NPI-Q mean comparisons and regression models adjusted by cognitive (Mini-Mental State Examination) and functional status (Clinical Dementia Rating Sum of Boxes) were performed to determine the effect of EOAD/LOAD and amnestic/non-amnestic diagnosis on NPI-Q. Regression models assessing the effect of co-pathologies on NPI-Q were performed.
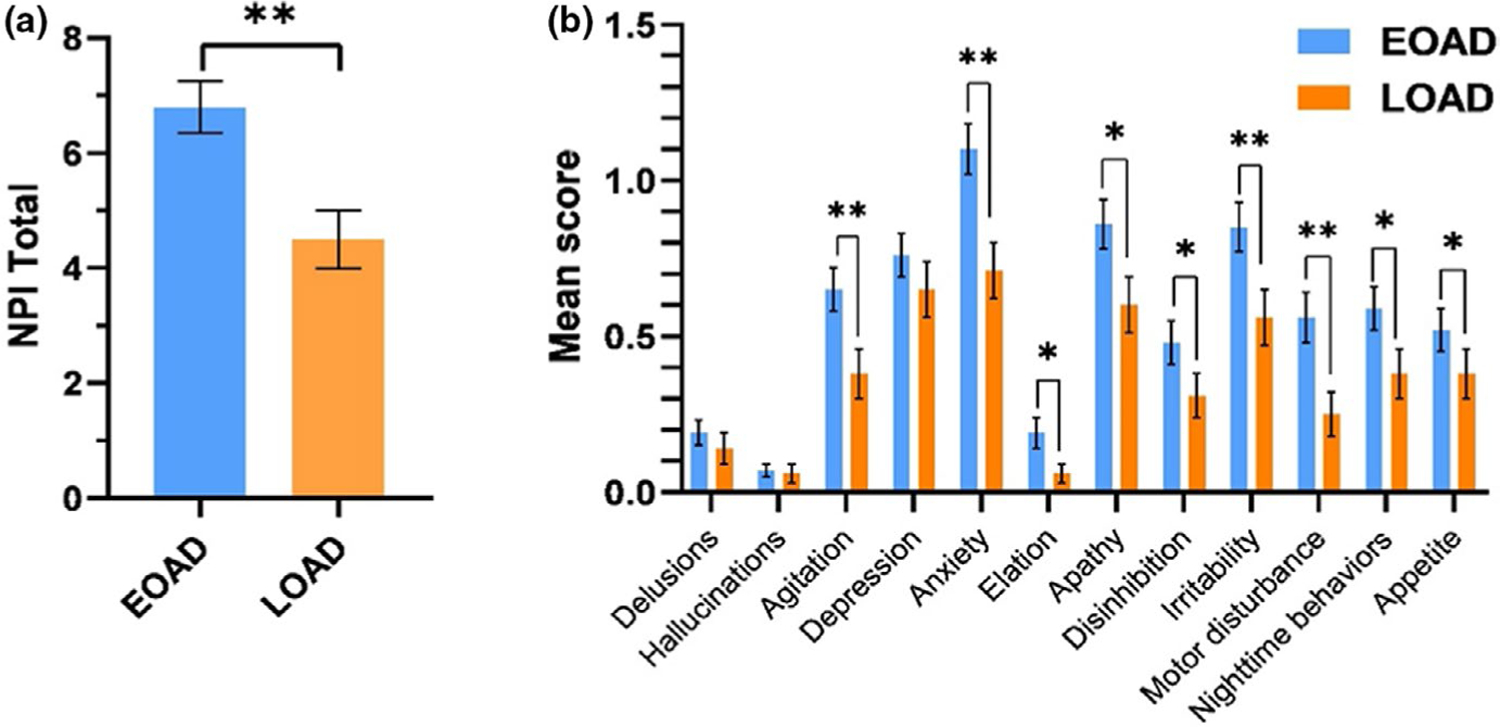
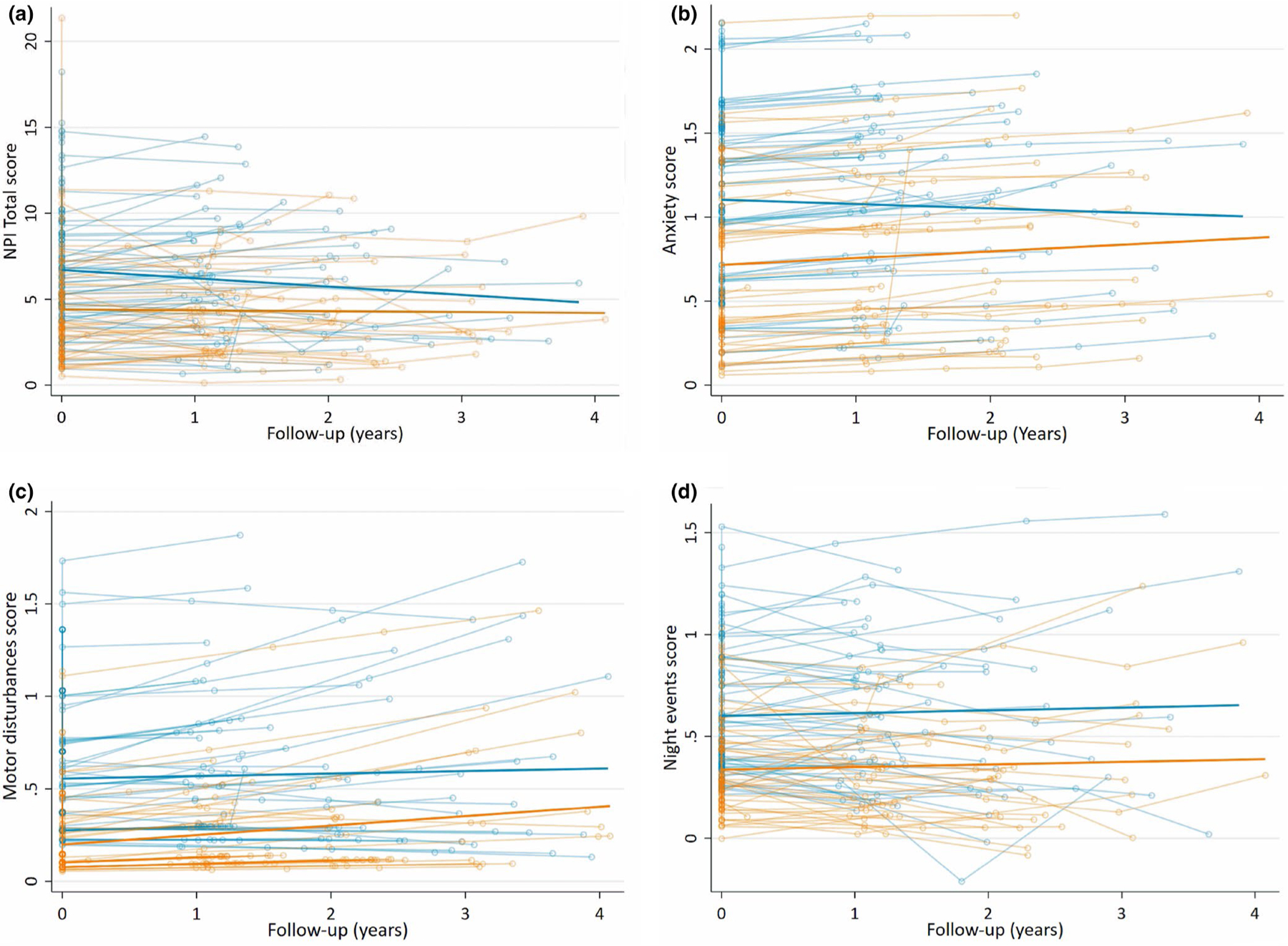
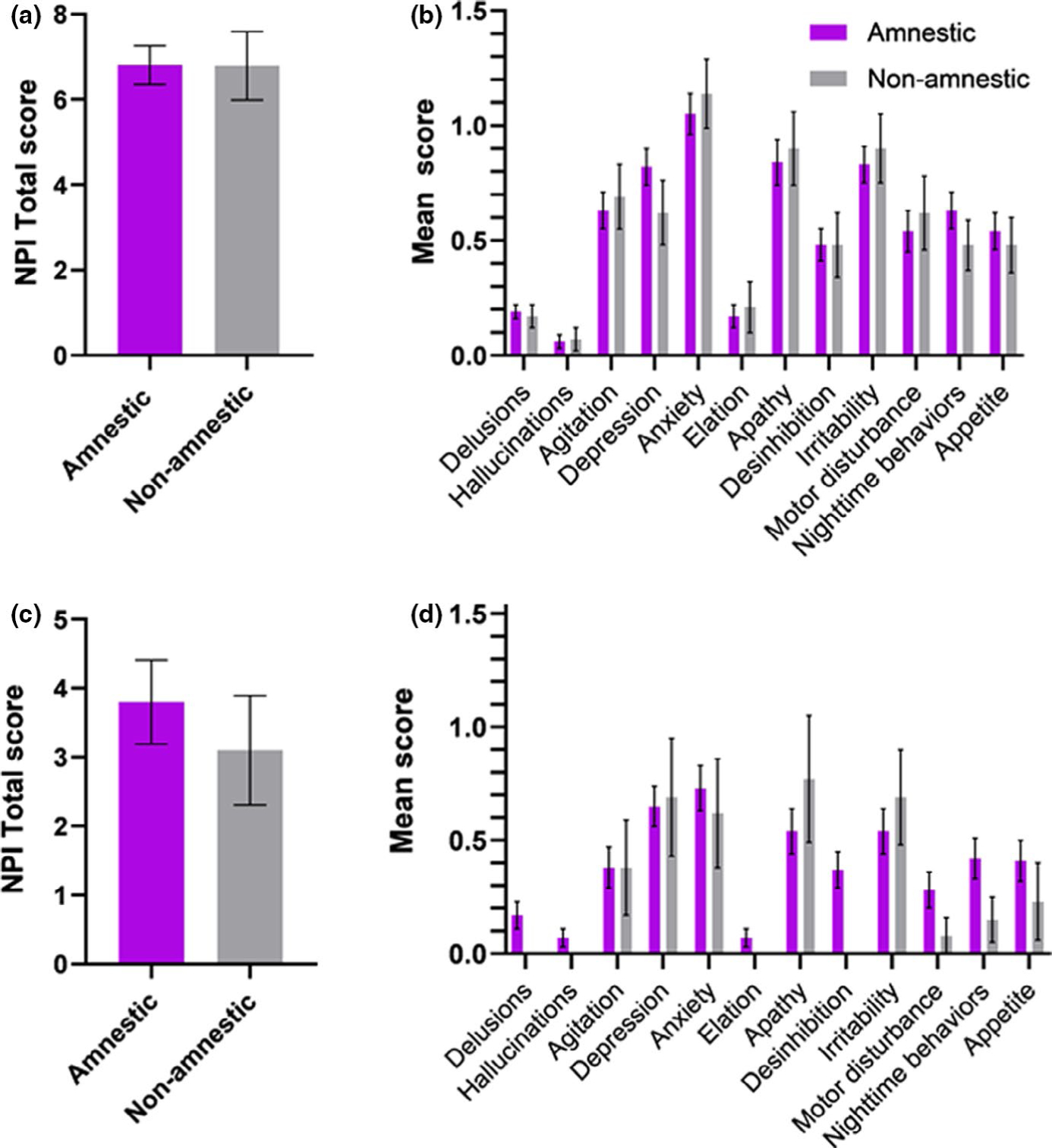
Results: At baseline, the NPI-Q scores were higher in EOAD compared to LOAD (p < 0.05). Longitudinally, regression models showed a significant effect of diagnosis, where EOAD had higher NPI-Q total, anxiety, motor disturbances and night-time behavior scores (p < 0.05). No differences between amnestics/non-amnestics were found. Argyrophilic grain disease co-pathology predicted a higher severity of NPI-Q scores in LOAD.
Conclusions: Anxiety, night-time behaviors and motor disturbances are more severe in EOAD than LOAD across the disease course. The differential patterns of neuropsychiatric symptoms observed between EOAD/LOAD could suggest a pattern of selective vulnerability extending to the brain's subcortical structures. Further, co-pathologies such as argyrophilic grain disease in LOAD may also play a role in increasing neuropsychiatric symptoms.
Keywords: Alzheimer's disease; behavioral symptoms; locus coeruleus; phenotype; sleep.
© 2021 European Academy of Neurology.
Conflict of interest statement
CONFLICT OF INTEREST
Authors declare no conflict of interest.
Figures
References
-
- Tanaka H, Hashimoto M, Fukuhara R, et al. Relationship between dementia severity and behavioural and psychological symptoms in early-onset Alzheimer’s disease. Psychogeriatrics 2015;15(4):242–247. - PubMed
