

Multiple health behaviour change primary care intervention for smoking cessation, physical activity and healthy diet in adults 45 to 75 years old (EIRA study): a hybrid effectiveness-implementation cluster randomised trial
- PMID: 34863136
- PMCID: PMC8642878
- DOI: 10.1186/s12889-021-11982-4
Multiple health behaviour change primary care intervention for smoking cessation, physical activity and healthy diet in adults 45 to 75 years old (EIRA study): a hybrid effectiveness-implementation cluster randomised trial
Abstract
Background: This study aimed to evaluate the effectiveness of a) a Multiple Health Behaviour Change (MHBC) intervention on reducing smoking, increasing physical activity and adherence to a Mediterranean dietary pattern in people aged 45-75 years compared to usual care; and b) an implementation strategy.
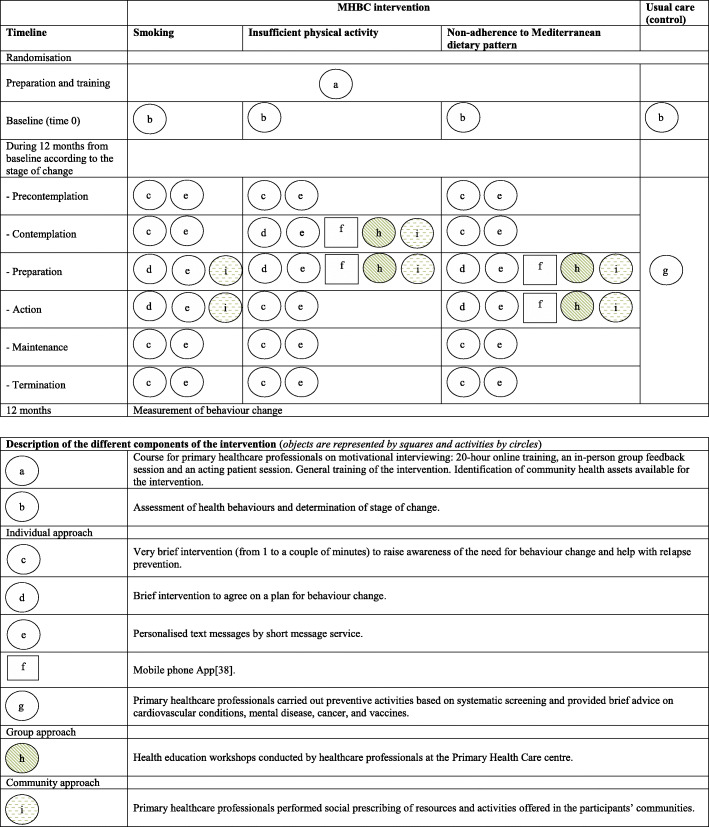
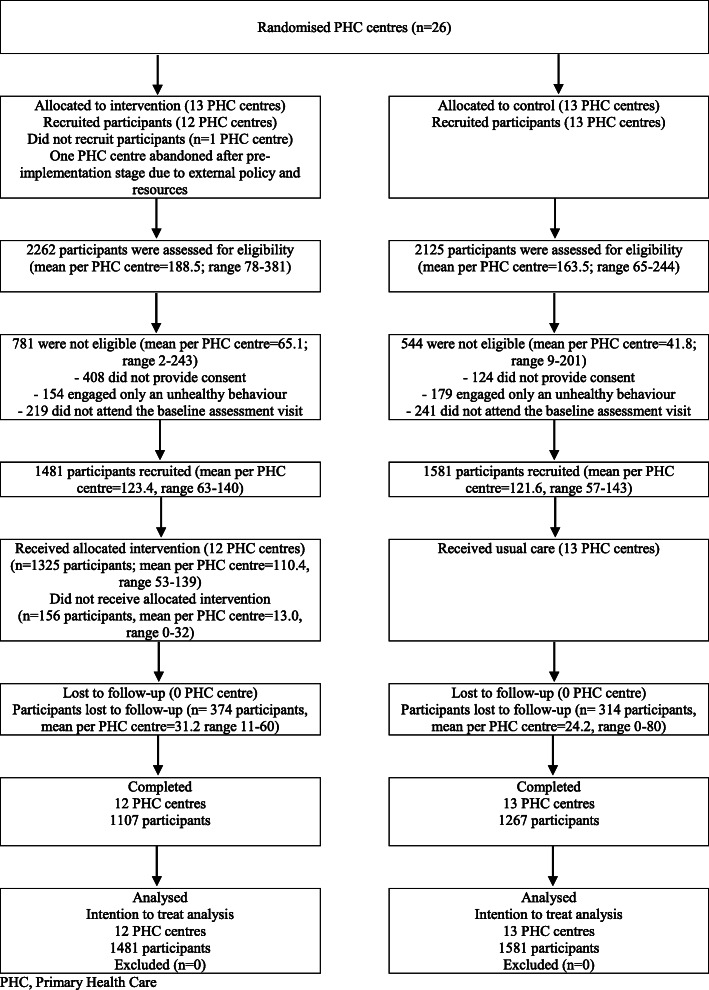
Methods: A cluster randomised effectiveness-implementation hybrid trial-type 2 with two parallel groups was conducted in 25 Spanish Primary Health Care (PHC) centres (3062 participants): 12 centres (1481 participants) were randomised to the intervention and 13 (1581 participants) to the control group (usual care). The intervention was based on the Transtheoretical Model and focused on all target behaviours using individual, group and community approaches. PHC professionals made it during routine care. The implementation strategy was based on the Consolidated Framework for Implementation Research (CFIR). Data were analysed using generalised linear mixed models, accounting for clustering. A mixed-methods data analysis was used to evaluate implementation outcomes (adoption, acceptability, appropriateness, feasibility and fidelity) and determinants of implementation success.
Results: 14.5% of participants in the intervention group and 8.9% in the usual care group showed a positive change in two or all the target behaviours. Intervention was more effective in promoting dietary behaviour change (31.9% vs 21.4%). The overall adoption rate by professionals was 48.7%. Early and final appropriateness were perceived by professionals as moderate. Early acceptability was high, whereas final acceptability was only moderate. Initial and final acceptability as perceived by the participants was high, and appropriateness moderate. Consent and recruitment rates were 82.0% and 65.5%, respectively, intervention uptake was 89.5% and completion rate 74.7%. The global value of the percentage of approaches with fidelity ≥50% was 16.7%. Eight CFIR constructs distinguished between high and low implementation, five corresponding to the Inner Setting domain.
Conclusions: Compared to usual care, the EIRA intervention was more effective in promoting MHBC and dietary behaviour change. Implementation outcomes were satisfactory except for the fidelity to the planned intervention, which was low. The organisational and structural contexts of the centres proved to be significant determinants of implementation effectiveness.
Trial registration: ClinicalTrials.gov , NCT03136211 . Registered 2 May 2017, "retrospectively registered".
Keywords: Health behaviour; Health promotion; Hybrid trial; Implementation science; Mediterranean diet; Physical activity; Primary health care; Smoking cessation.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization [Internet]. Geneva: World Health Organization; 2019 [cited 2019 Dec 12]. Global Health Observatory (GHO) data. Deaths from NCDs [Internet] Available from: https://www.who.int/gho/ncd/mortality_morbidity/ncd_total/en/
-
- World Health Organization . Global status report on noncommunicable diseases 2014. Geneva: World Health Organization; 2014.
-
- World Health Organization (WHO). Global action plan for the prevention and control of noncommunicable diseases 2013-2020. Geneva: WHO; 2013. Available from: https://apps.who.int/iris/bitstream/handle/10665/94384/9789241506236_eng...
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
