

Endovascular revascularization strategies using catheter-based thrombectomy versus conventional catheter-directed thrombolysis for acute limb ischemia
- PMID: 34863195
- PMCID: PMC8645071
- DOI: 10.1186/s12959-021-00349-9
Endovascular revascularization strategies using catheter-based thrombectomy versus conventional catheter-directed thrombolysis for acute limb ischemia
Abstract
Background: Acute limb ischemia (ALI) is an important clinical event threatening both life and the affected limbs, but the optimal treatment for ALI remains undefined. The aim of this study was to compare the safety and effectiveness of thrombectomy approaches via either catheter-based thrombectomy (CBT) or catheter-directed thrombolysis (CDT).
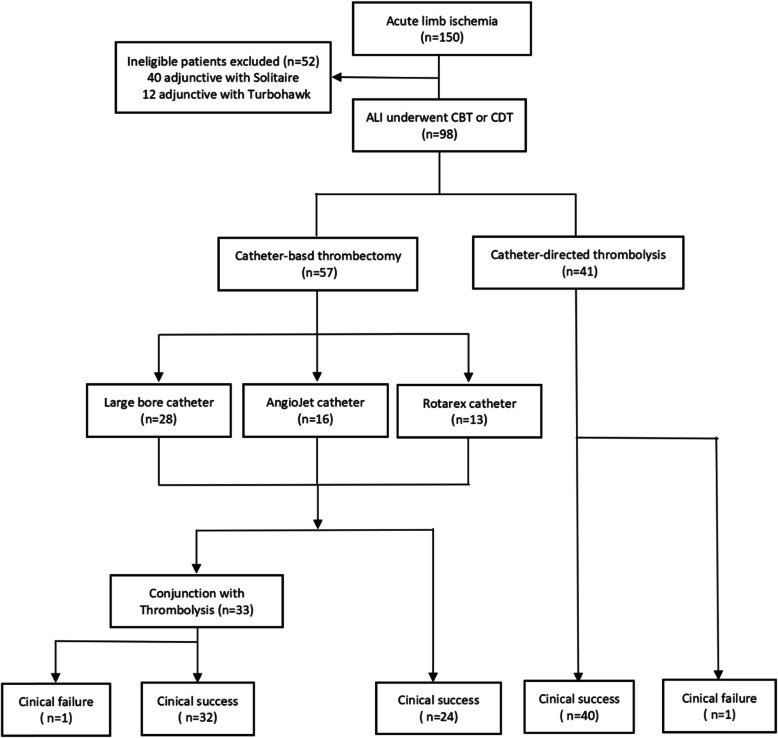
Methods: A total of 98 patients (mean age 69.7 years, 60 male) who underwent endovascular intervention for ALI from January 2015 to July 2019 were included. Of these, 57 were treated with primary CBT via a large-bore catheter, an AngioJet catheter or Rotarex catheter, and/or underwent low-dose CDT, and 41 were treated with primary CDT. The safety and effectiveness of CBT compared to conventional CDT and other various endovascular techniques were evaluated.
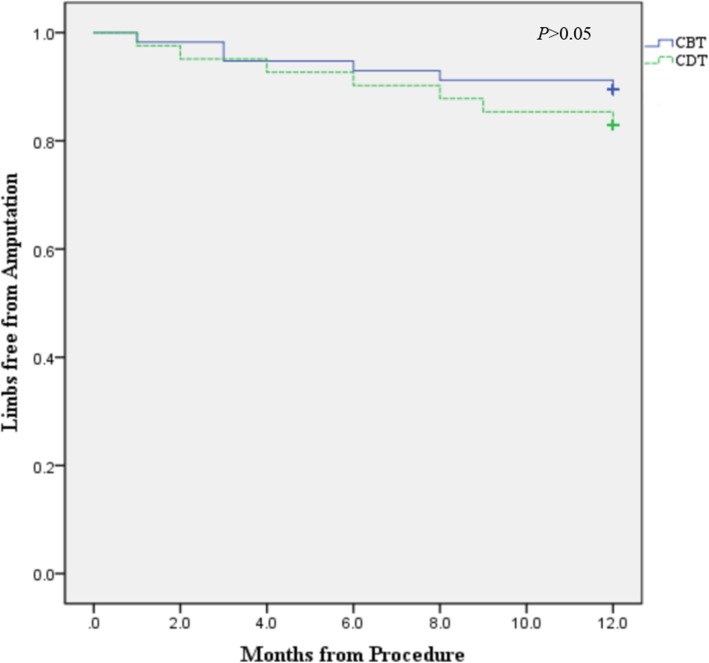
Results: More Rutherford IIb patients were treated with primary CBT (68.4%) than CDT (26.8%; P < .001). Patients who underwent primary CDT achieved a higher technical success rate than those who underwent primary CBT in a shorter procedure time (P < .001), whereas 42.1% of patients who underwent CBT did not need adjunctive CDT. The duration and dosage of adjunctive CDT in the CBT group were significantly decreased compared with those in the primary CDT group (both P < .001), and the CBT group achieved a shorter in-hospital length of stay (P < .001). Subgroup analysis revealed that patients treated with AngioJet and Rotarex catheters achieved slightly lower dosages, shorter CDT durations and shorter in-hospital stay lengths than those treated with large-bore catheters (P > .05). Clinical success was estimated to be achieved in 98.2% of patients who underwent CBT, which is similar to the 97.6% estimated in those who underwent primary CDT (P = 1.000), and this finding was similar among the CBT subgroups. Patients who underwent CBT had a higher procedure-related distal embolization rate and economic cost than those who underwent primary CDT (P < .05), but it had slightly fewer complications than those who underwent primary CDT (P = .059), especially minor complications (P = .036). The freedom from amputation at 6 and 12 months for CBT and CDT was assessed (93.0% vs 90.2% respectively, P = .625; 89.5% vs 82.9%, respectively, P = .34,). Comparable limb salvage was found for different techniques of large bore catheters, AngioJet catheters and Rotarex catheters. The Kaplan-Meier table analysis also showed similar limb salvage rates between groups.
Conclusions: Endovascular treatment of ALI with the use of catheter-based therapies is an effective modality that can reduce the requirement for thrombolysis, with expected reductions in hemorrhagic complications, but at the risk of remediable distal emboli and increased economic cost. It has a similar clinical outcome to conventional CDT alone. Different CBT techniques have comparable efficacy but different adverse event profiles.
Keywords: Acute limb ischemia; Catheter-based thrombectomy; Catheter-directed thrombolysis; Endovascular treatment; Percutaneous mechanical thrombectomy.
© 2021. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article. The content of the manuscript is original, and it has not been published or accepted for publication.
Figures
References
-
- Björck M, Earnshaw JJ, Acosta S, Bastos Gonçalves F, Cochennec F, Debus ES, Hinchliffe R, Jongkind V, Koelemay MJW, Menyhei G, Svetlikov AV, Tshomba Y, van den Berg JC, ESVS Guidelines Committee, de Borst GJ, Chakfé N, Kakkos SK, Koncar I, Lindholt JS, Tulamo R, Vega de Ceniga M, Vermassen F, Document Reviewers, Boyle JR, Mani K, Azuma N, Choke ETC, Cohnert TU, Fitridge RA, Forbes TL, Hamady MS, Munoz A, Müller-Hülsbeck S, Rai K. Editor's choice-European Society for Vascular Surgery (ESVS) 2020 clinical practice guidelines on the management of acute limb ischaemia. Eur J Vasc Endovasc Surg. 2020;59(2):173–218. doi: 10.1016/j.ejvs.2019.09.006. - DOI - PubMed
-
- Hess CN, Huang Z, Patel MR, Baumgartner I, Berger JS, Blomster JI, Fowkes FGR, Held P, Jones WS, Katona B, Mahaffey KW, Norgren L, Rockhold FW, Hiatt WR. Acute limb ischemia in peripheral artery disease: insights from EUCLID. Circulation. 2019;140(7):556–565. doi: 10.1161/CIRCULATIONAHA.119.039773. - DOI - PubMed
-
- Howard DP, Banerjee A, Fairhead JF, Hands L, Silver LE, Rothwell PM. Population-based study of incidence, risk factors, outcome, and prognosis of ischemic peripheral arterial events: implications for prevention. Circulation. 2015;132(19):1805–1815. doi: 10.1161/CIRCULATIONAHA.115.016424. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
