

Elevated CSF inflammatory markers in patients with idiopathic normal pressure hydrocephalus do not promote NKCC1 hyperactivity in rat choroid plexus
- PMID: 34863228
- PMCID: PMC8645122
- DOI: 10.1186/s12987-021-00289-6
Elevated CSF inflammatory markers in patients with idiopathic normal pressure hydrocephalus do not promote NKCC1 hyperactivity in rat choroid plexus
Abstract
Background: Idiopathic normal pressure hydrocephalus (iNPH) is a potentially reversible neurological condition of unresolved etiology characterized by a clinical triad of symptoms; gait disturbances, urinary incontinence, and cognitive deterioration. In the present study, we aimed to elucidate the molecular coupling between inflammatory markers and development of iNPH and determine whether inflammation-induced hyperactivity of the choroidal Na+/K+/2Cl- cotransporter (NKCC1) that is involved in cerebrospinal fluid (CSF) secretion could contribute to the iNPH pathogenesis.
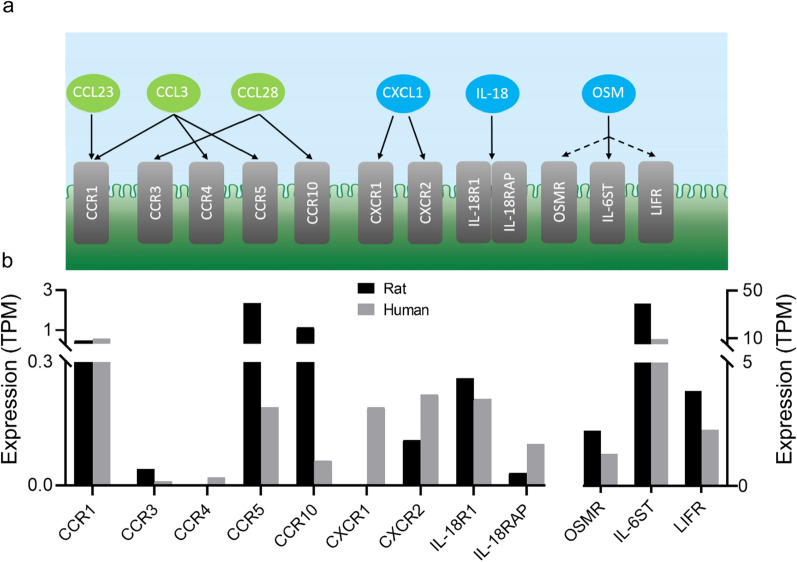
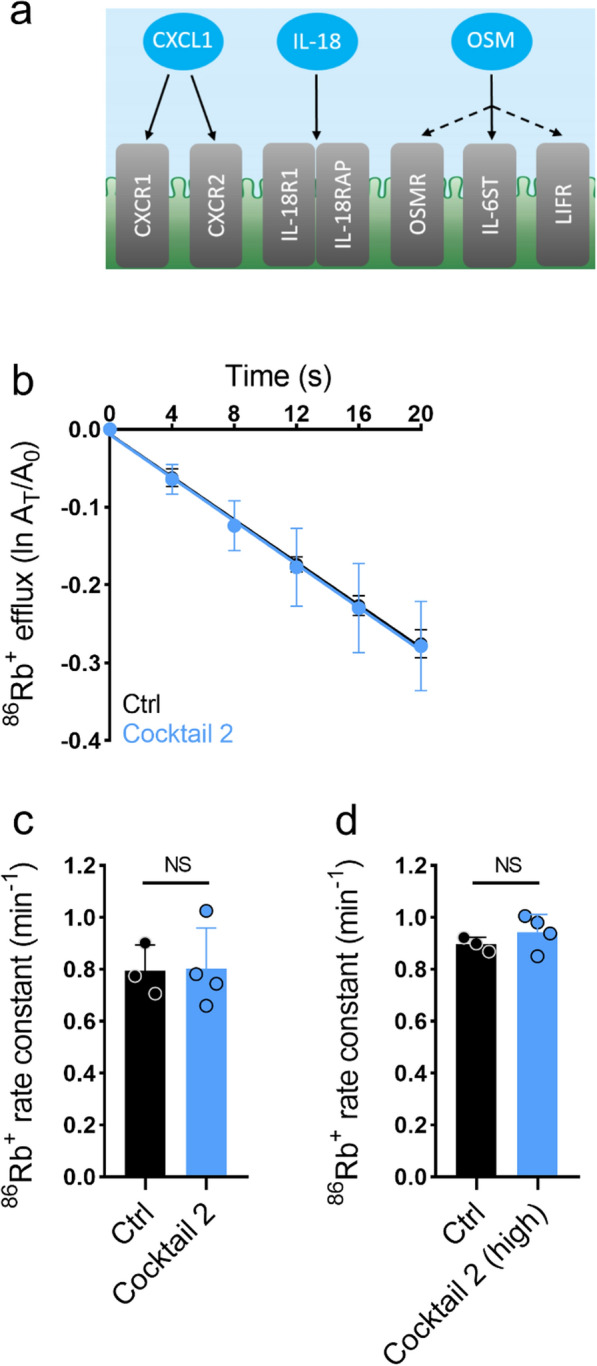
Methods: Lumbar CSF samples from 20 iNPH patients (10 with clinical improvement upon CSF shunting, 10 without clinical improvement) and 20 elderly control subjects were analyzed with the novel proximity extension assay technique for presence of 92 different inflammatory markers. RNA-sequencing was employed to delineate choroidal abundance of the receptors for the inflammatory markers found elevated in the CSF from iNPH patients. The ability of the elevated inflammatory markers to modulate choroidal NKCC1 activity was determined by addition of combinations of rat version of these in ex vivo experiments on rat choroid plexus.
Results: 11 inflammatory markers were significantly elevated in the CSF from iNPH patients compared to elderly control subjects: CCL28, CCL23, CCL3, OPG, CXCL1, IL-18, IL-8, OSM, 4E-BP1, CXCL6, and Flt3L. One inflammatory marker, CDCP1, was significantly decreased in iNPH patients compared to control subjects. None of the inflammatory markers differed significantly when comparing iNPH patients with and without clinical improvement upon CSF shunting. All receptors for the elevated inflammatory markers were expressed in the rat and human choroid plexus, except CCR4 and CXCR1, which were absent from the rat choroid plexus. None of the elevated inflammatory markers found in the CSF from iNPH patients modulated the choroidal NKCC1 activity in ex vivo experiments on rat choroid plexus.
Conclusion: The CSF from iNPH patients contains elevated levels of a subset of inflammatory markers. Although the corresponding inflammatory receptors are, in general, expressed in the choroid plexus of rats and humans, their activation did not modulate the NKCC1-mediated fraction of choroidal CSF secretion ex vivo. The molecular mechanisms underlying ventriculomegaly in iNPH, and the possible connection to inflammation, therefore remains to be elucidated.
Keywords: Biomarkers; Cerebrospinal fluid; Choroid plexus; Inflammatory marker; Normal pressure hydrocephalus.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Hakim S, Adams RD. The special clinical problem of symptomatic hydrocephalus with normal cerebrospinal fluid pressure. J Neurol Sci. 1965;2:307–327. - PubMed
-
- Relkin N, Marmarou A, Klinge P, Bergsneider M, Black PM. Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery. 2005;57:S4–16. - PubMed
-
- Hebb AO, Cusimano MD. Idiopathic normal pressure hydrocephalus: a systematic review of diagnosis and outcome. Neurosurgery. 2001;49:1166–1186. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
