

Quantification of Glomerular Structural Lesions: Associations With Clinical Outcomes and Transcriptomic Profiles in Nephrotic Syndrome
- PMID: 34864148
- PMCID: PMC10795715
- DOI: 10.1053/j.ajkd.2021.10.004
Quantification of Glomerular Structural Lesions: Associations With Clinical Outcomes and Transcriptomic Profiles in Nephrotic Syndrome
Abstract
Rationale & objective: The current classification system for focal segmental glomerulosclerosis (FSGS) and minimal change disease (MCD) does not fully capture the complex structural changes in kidney biopsies nor the clinical and molecular heterogeneity of these diseases.
Study design: Prospective observational cohort study.
Setting & participants: 221 MCD and FSGS patients enrolled in the Nephrotic Syndrome Study Network (NEPTUNE).
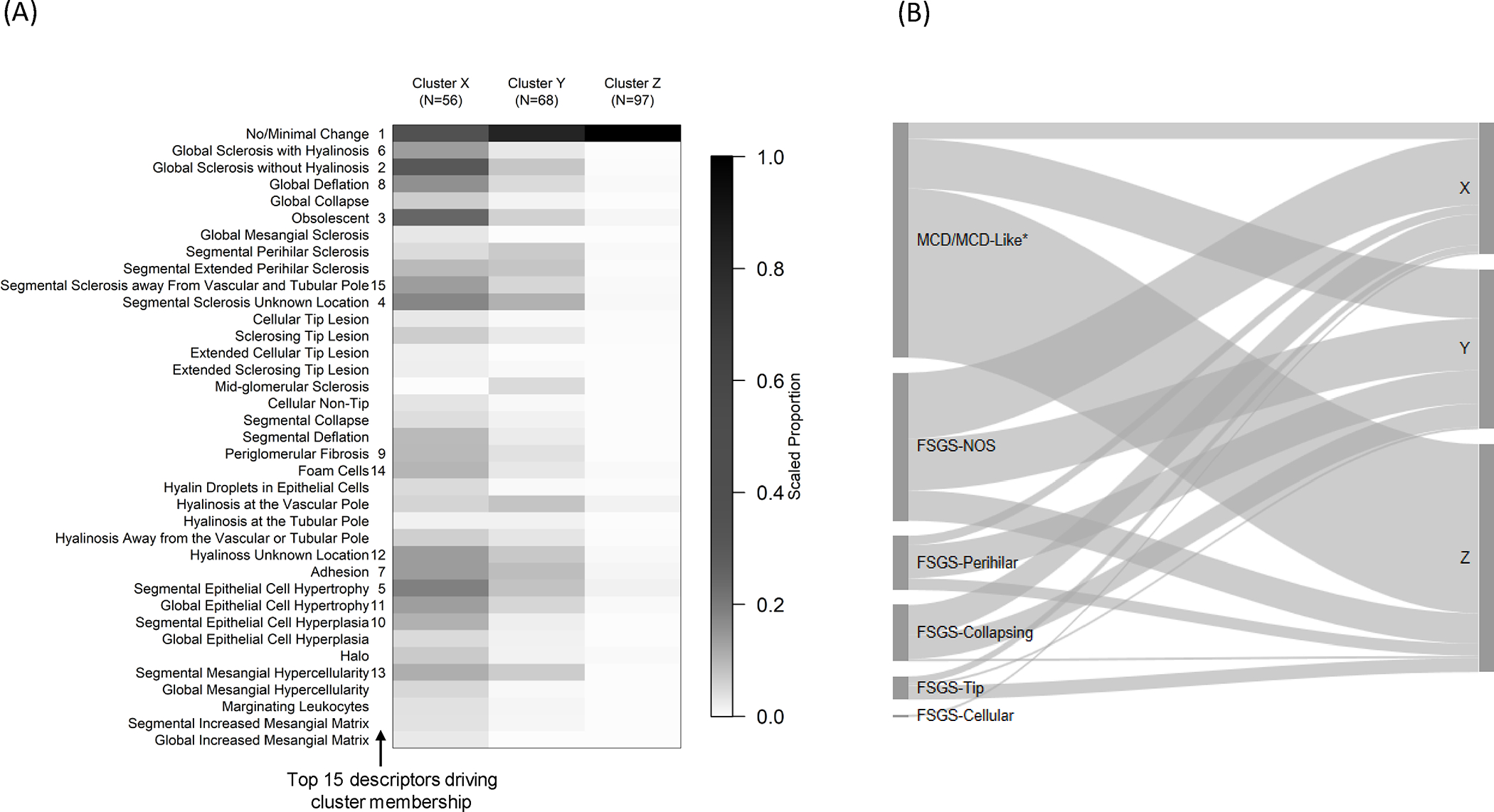
Exposure: The NEPTUNE Digital Pathology Scoring System (NDPSS) was applied to generate scores for 37 glomerular descriptors.
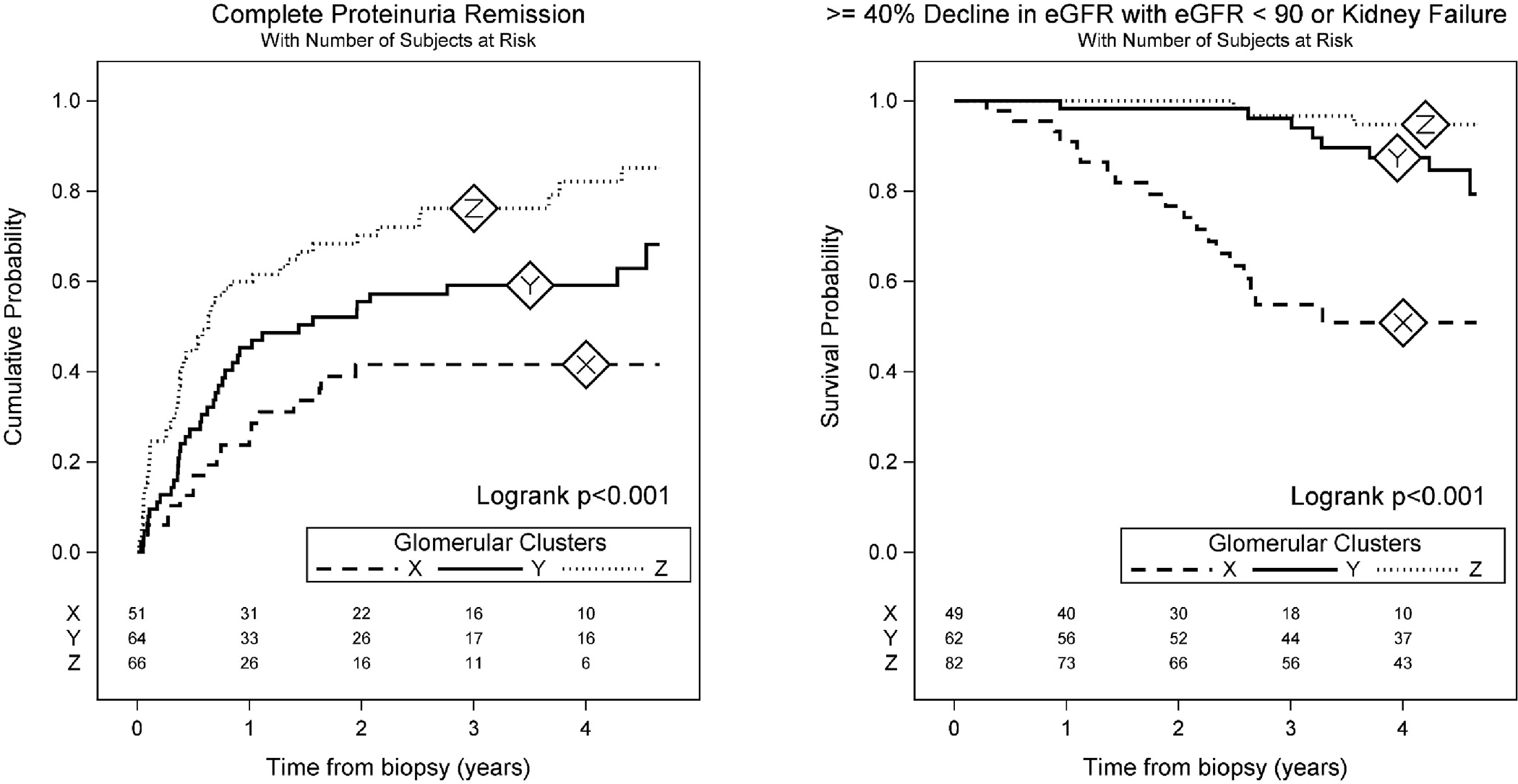
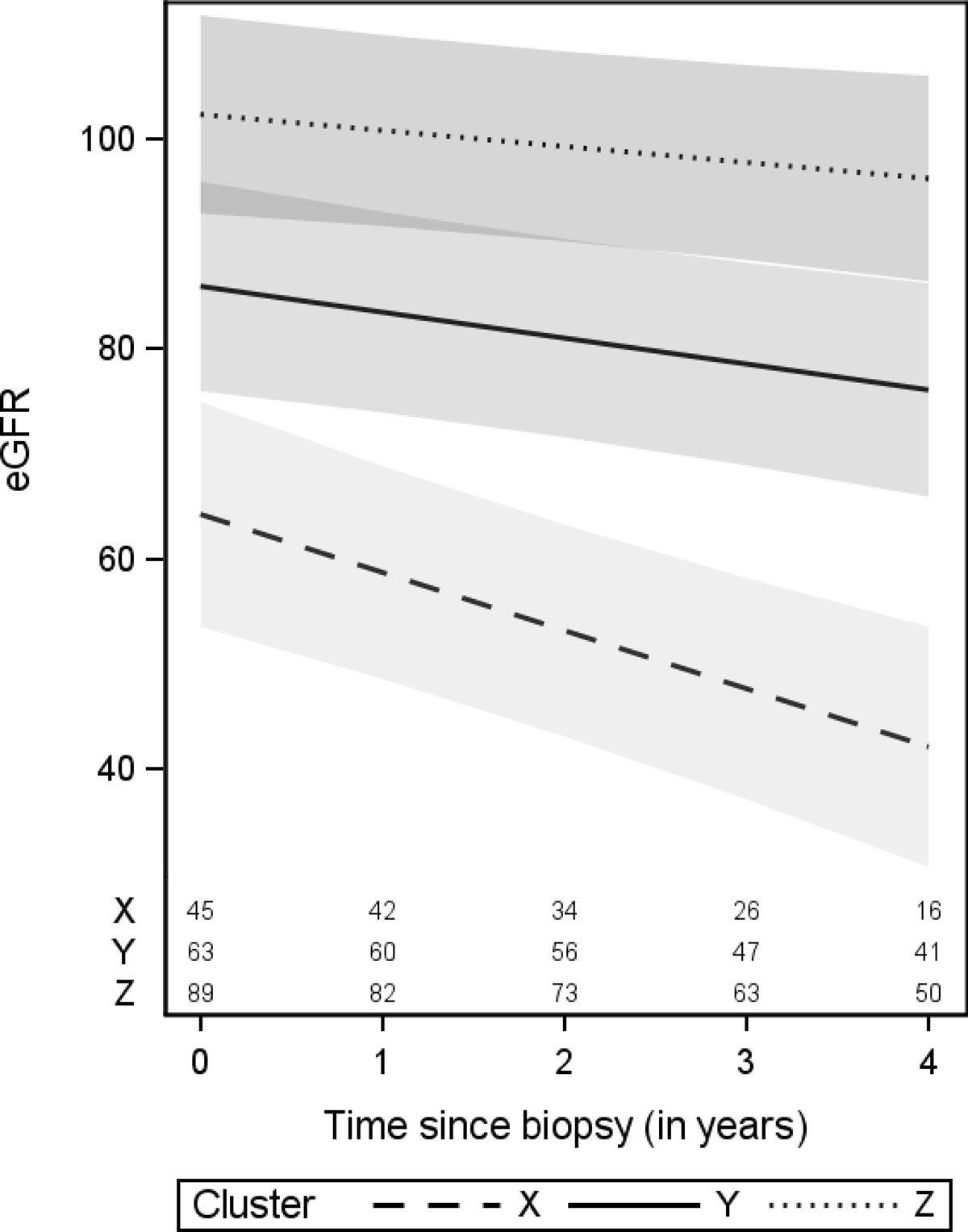
Outcome: Time from biopsy to complete proteinuria remission, time from biopsy to kidney disease progression (40% estimated glomerular filtration rate [eGFR] decline or kidney failure), and eGFR over time.
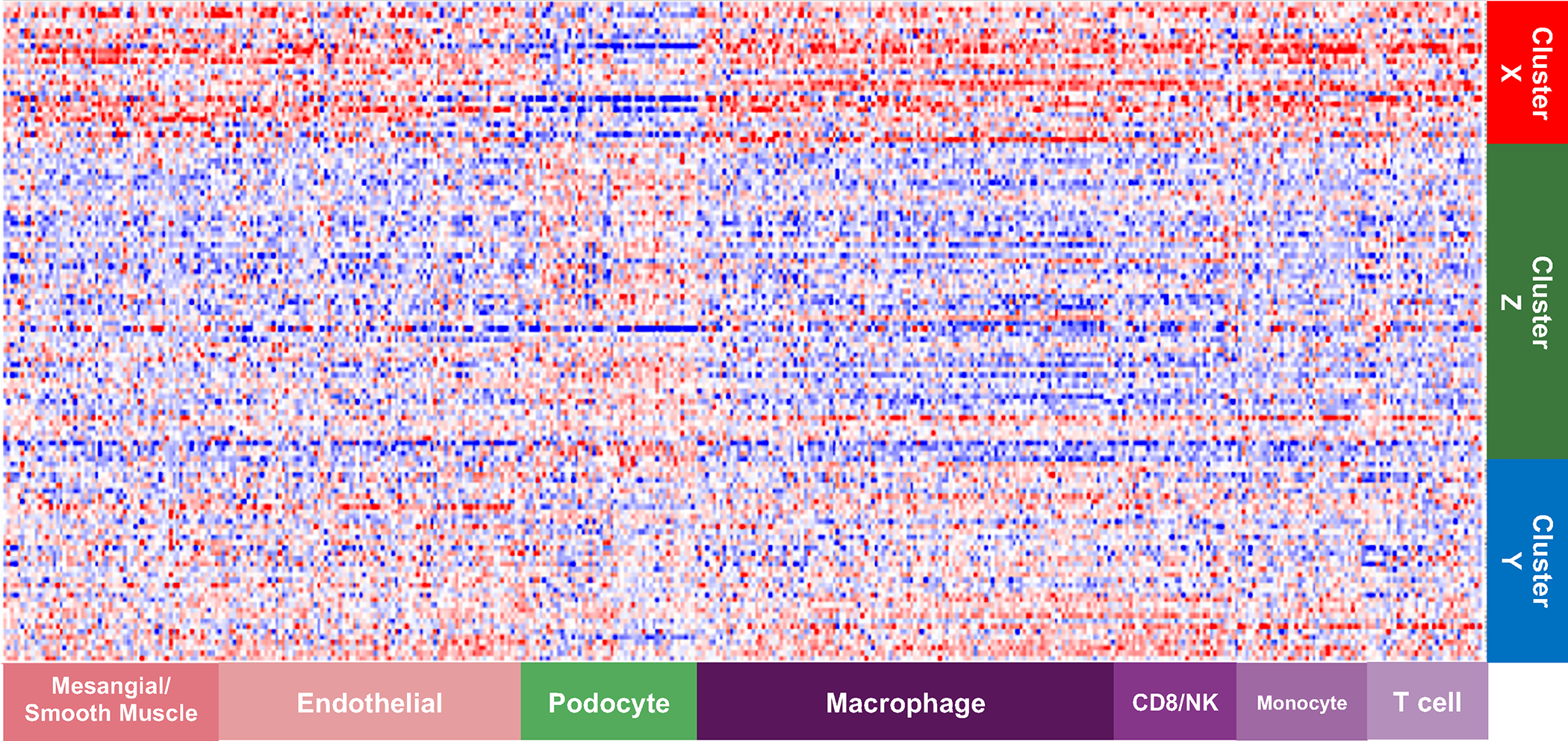
Analytical approach: Cluster analysis was used to group patients with similar morphologic characteristics. Glomerular descriptors and patient clusters were assessed for associations with outcomes using adjusted Cox models and linear mixed models. Messenger RNA from glomerular tissue was used to assess differentially expressed genes between clusters and identify genes associated with individual descriptors driving cluster membership.
Results: Three clusters were identified: X (n = 56), Y (n = 68), and Z (n = 97). Clusters Y and Z had higher probabilities of proteinuria remission (HRs of 1.95 [95% CI, 0.99-3.85] and 3.29 [95% CI, 1.52-7.13], respectively), lower hazards of disease progression (HRs of 0.22 [95% CI, 0.08-0.57] and 0.11 [95% CI, 0.03-0.45], respectively), and lower loss of eGFR over time compared with X. Cluster X had 1,920 genes that were differentially expressed compared with Y+Z; these reflected activation of pathways of immune response and inflammation. Six descriptors driving the clusters individually correlated with clinical outcomes and gene expression.
Limitations: Low prevalence of some descriptors and biopsy at a single time point.
Conclusions: The NDPSS allows for categorization of FSGS/MCD patients into clinically and biologically relevant subgroups, and uncovers histologic parameters associated with clinical outcomes and molecular signatures not included in current classification systems.
Keywords: Clinical outcomes; disease classification; focal segmental glomerulosclerosis (FSGS); gene expression; glomerular disease; glomerular structure; kidney biopsy; minimal change disease (MCD); molecular analysis; morphologic features; nephrotic syndrome; precision medicine; proteinuria; renal pathology; transcriptomics.
Copyright © 2022. Published by Elsevier Inc.
Figures
Comment in
-
Outscoring Current Classification Systems for Nephrotic Syndrome.Am J Kidney Dis. 2022 Jun;79(6):783-784. doi: 10.1053/j.ajkd.2021.12.005. Epub 2022 Feb 10. Am J Kidney Dis. 2022. PMID: 35153081 No abstract available.
References
-
- D’Agati VD, Fogo AB, Bruijn JA, Jennette JC. Pathologic classification of focal segmental glomerulosclerosis: a working proposal. Am J Kidney Dis. 2004:368–82. vol. 2. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
