

Unclear retroperitoneal tumors, an interdisciplinary challenge - A case report and review of the literature
- PMID: 34864261
- PMCID: PMC8645916
- DOI: 10.1016/j.ijscr.2021.106634
Unclear retroperitoneal tumors, an interdisciplinary challenge - A case report and review of the literature
Abstract
Introduction and importance: Unclear retroperitoneal tumors impose major challenges for clinicians. Tumors can originate primarily from retroperitoneal tissue or secondarily invade into the retroperitoneum. While benign lesions also occur, malignant tumors are far more common. Clinical presentation depends on replacement or invasion of other organs and is therefore highly variable. The heterogeneous tumor composition makes a definitive preoperative diagnosis difficult. Surgical resection is the gold standard for treatment but often proves challenging due to frequent involvement of large retroperitoneal vessels.
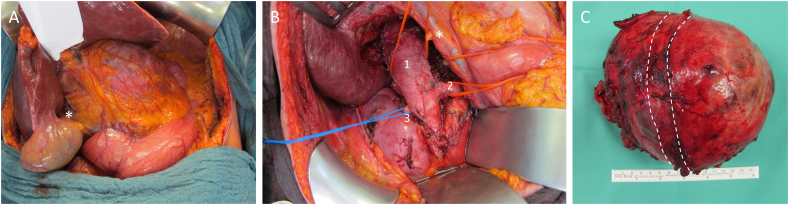
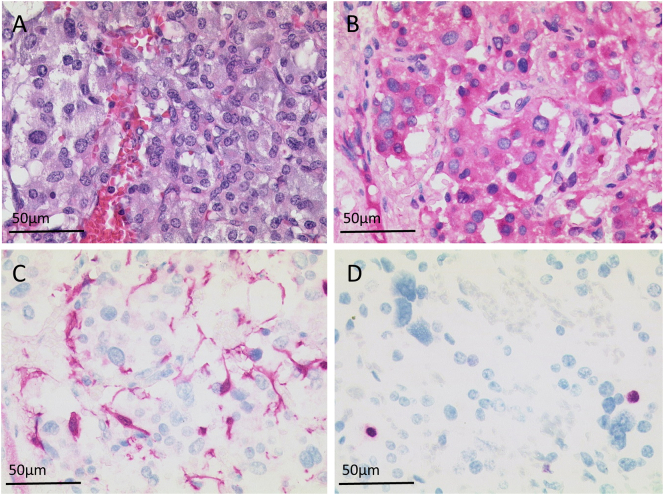
Case presentation: We present the case of a 70-year old woman diagnosed with a large, unclear retroperitoneal tumor. Initial clinical symptoms were increasing dyspnea and dysphagia in our clinic. Gastroenterologic and cardiologic workup was unremarkable. Computed Tomography (CT) revealed a large retroperitoneal mass in the right upper abdomen with severe displacement of the inferior vena cava and renal veins. The patient was scheduled for primary tumor resection. The procedure was challenging due to the vessel involvement and large blood pressure alterations during tumor mobilization. The post-op pathologic workup then revealed the rare finding of a completely resected paraganglioma. The post-surgical course was uneventful. One year after diagnosis, the patient is relapse-free.
Clinical discussion: Among retroperitoneal tumors, paragangliomas and pheochromocytomas are rare tumor entities. Asymptomatic, sporadic disease is hard to identify preoperatively and can cause unexpected complications in the OR. An experienced team is crucial in achieving best short- and long-term outcomes.
Conclusion: This case impressively shows the challenges of retroperitoneal tumors and the importance of interdisciplinary work in these cases.
Keywords: Case report; PPGL; Paraganglioma; Pheochromocytoma; Retroperitoneal tumor; Surgery.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Agha R.A., Franchi T., Sohrabi C., Mathew G., Kerwan A., Thoma A., Beamish A.J., Noureldin A., Rao A., Vasudevan B., The S.C.A.R.E. Guideline: updating consensus surgical CAse REport (SCARE) guidelines. Int. J. Surg. 2020;84(2020):226–230. - PubMed
-
- Rajiah P., Sinha R., Cuevas C., Dubinsky T.J., Bush W.H., Jr., Kolokythas O. Imaging of uncommon retroperitoneal masses. Radiographics. 2011;31:949–976. - PubMed
-
- Lee K.Y., Oh Y., Noh H.J., Lee Y.J., Yong H., Kang E., Kim K.A., Lee N.J. Extraadrenal paragangliomas of the body: imaging features. Am. J. Roentgenol. 2006;187:492–504. - PubMed
-
- Kimura N., Takayanagi R., Takizawa N., Itagaki E., Katabami T., Kakoi N., Rakugi H., Ikeda Y., Tanabe A., Nigawara T. Pathological grading for predicting metastasis in phaeochromocytoma and paraganglioma. Endocr. Relat. Cancer. 2014;21:405–414. - PubMed
-
- Niemeijer N., Alblas G., Van Hulsteijn L., Dekkers O., Corssmit E. Chemotherapy with cyclophosphamide, vincristine and dacarbazine for malignant paraganglioma and pheochromocytoma: systematic review and meta-analysis. Clin. Endocrinol. 2014;81:642–651. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
