

Lethal Pediatric Cerebral Vasculitis Triggered by Severe Acute Respiratory Syndrome Coronavirus 2
- PMID: 34864371
- PMCID: PMC8585961
- DOI: 10.1016/j.pediatrneurol.2021.11.003
Lethal Pediatric Cerebral Vasculitis Triggered by Severe Acute Respiratory Syndrome Coronavirus 2
Abstract
Background: We report the clinical, radiological, laboratory, and neuropathological findings in support of the first diagnosis of lethal, small-vessel cerebral vasculitis triggered by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in a pediatric patient.
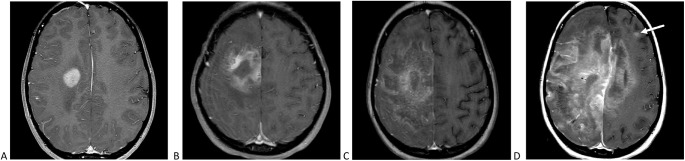
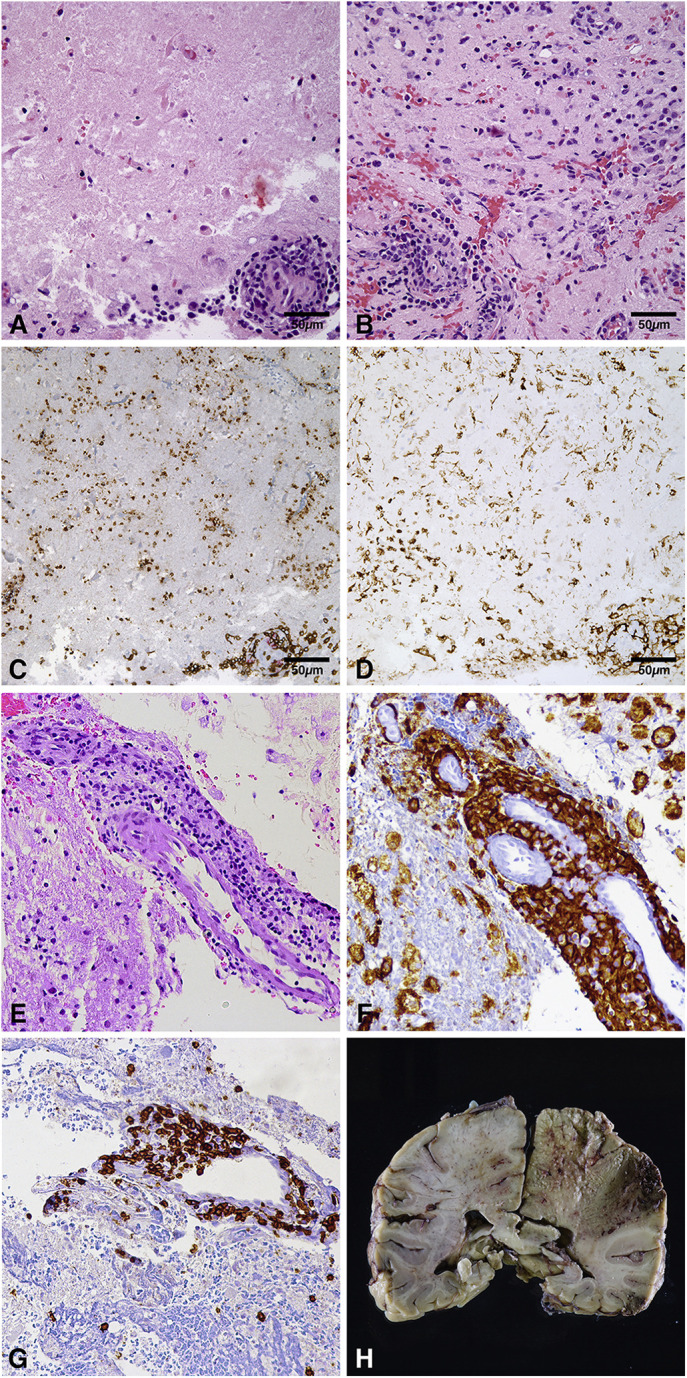
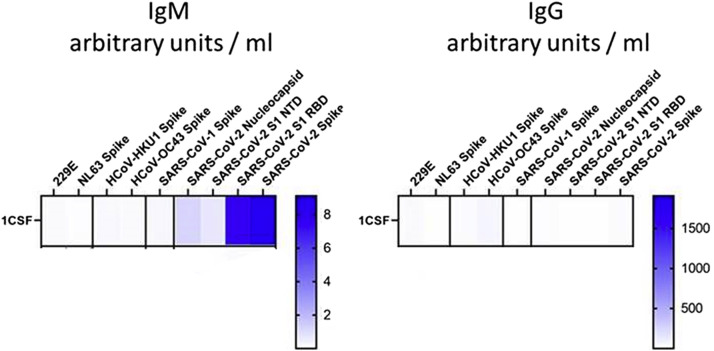
Patient description: A previously healthy, eight-year-old Hispanic girl presented with subacute left-sided weakness two weeks after a mild febrile illness. SARS-CoV-2 nasopharyngeal swab was positive. Magnetic resonance imaging revealed an enhancing right frontal lobe lesion with significant vasogenic edema. Two brain biopsies of the lesion showed perivascular and intraluminal lymphohistiocytic inflammatory infiltrate consistent with vasculitis. Despite extensive treatment with immunomodulatory therapies targeting primary angiitis of the central nervous system, she experienced neurological decline and died 93 days after presentation. SARS-CoV-2 testing revealed positive serum IgG and positive cerebrospinal fluid IgM. Comprehensive infectious, rheumatologic, hematologic/oncologic, and genetic evaluation did not identify an alternative etiology. Postmortem brain autopsy remained consistent with vasculitis.
Conclusion: This is the first pediatric presentation to suggest that SARS-CoV-2 can lead to a fatal, postinfectious, inflammatory small-vessel cerebral vasculitis. Our patient uniquely included supportive cerebrospinal fluid and postmortem tissue analysis. While most children recover from the neurological complications of SARS-CoV-2, we emphasize the potential mortality in a child with no risk factors for severe disease.
Keywords: COVID-19; Cerebral vasculitis; Pediatrics; SARS-CoV-2; Stroke.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
References
-
- Hanumanthe S.B., Francisco C., Hart J., Graves J., Waubant E. Biopsy-supported tumefactive demyelination of the central nervous system in children. J Child Neurol. 2016;31:1528–1533. - PubMed
-
- Elbers J., Halliday W., Hawkins C., Hutchinson C., Benseler S.M. Brain biopsy in children with primary small-vessel central nervous system vasculitis. Ann Neurol. 2010;68:602–610. - PubMed
-
- Salvarani C., Brown R.D., Christianson T.J.H., et al. Primary central nervous system vasculitis mimicking brain tumor: comprehensive analysis of 13 cases from a single institutional cohort of 191 cases. J Autoimmun. 2019;97:22–28. - PubMed
-
- Denny A.M., Das S.K. A case of central nervous system vasculitis presenting as a mass-like lesion. Childs Nerv Syst. 2019;35:1223–1226. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
