

Prevalence of Mycobacterium tuberculosis in Sputum and Reported Symptoms Among Clinic Attendees Compared With a Community Survey in Rural South Africa
- PMID: 34864910
- PMCID: PMC9410725
- DOI: 10.1093/cid/ciab970
Prevalence of Mycobacterium tuberculosis in Sputum and Reported Symptoms Among Clinic Attendees Compared With a Community Survey in Rural South Africa
Erratum in
-
Correction to: Prevalence of Mycobacterium tuberculosis in Sputum and Reported Symptoms Among Clinic Attendees Compared With a Community Survey in Rural South Africa.Clin Infect Dis. 2022 Aug 25;75(2):363. doi: 10.1093/cid/ciac244. Clin Infect Dis. 2022. PMID: 35477792 Free PMC article. No abstract available.
Abstract
Background: Tuberculosis (TB) case finding efforts typically target symptomatic people attending health facilities. We compared the prevalence of Mycobacterium tuberculosis (Mtb) sputum culture-positivity among adult clinic attendees in rural South Africa with a concurrent, community-based estimate from the surrounding demographic surveillance area (DSA).
Methods: Clinic: Randomly selected adults (≥18 years) attending 2 primary healthcare clinics were interviewed and requested to give sputum for mycobacterial culture. Human immunodeficiency virus (HIV) and antiretroviral therapy (ART) status were based on self-report and record review. Community: All adult (≥15 years) DSA residents were invited to a mobile clinic for health screening, including serological HIV testing; those with ≥1 TB symptom (cough, weight loss, night sweats, fever) or abnormal chest radiograph were asked for sputum.
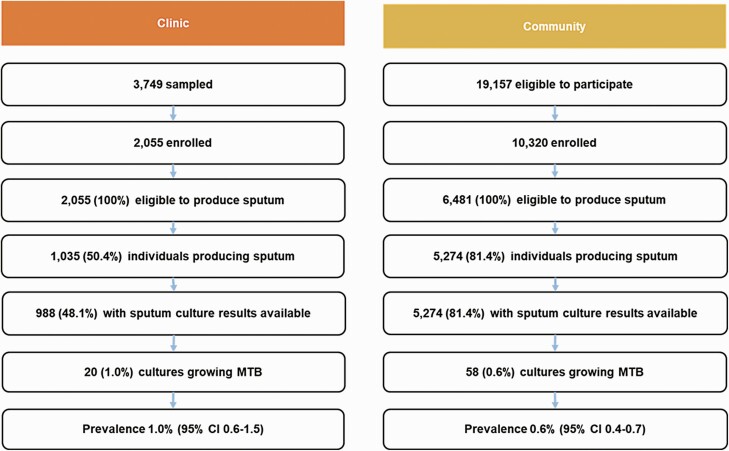
Results: Clinic: 2055 patients were enrolled (76.9% female; median age, 36 years); 1479 (72.0%) were classified HIV-positive (98.9% on ART) and 131 (6.4%) reported ≥1 TB symptom. Of 20/2055 (1.0% [95% CI, .6-1.5]) with Mtb culture-positive sputum, 14 (70%) reported no symptoms. Community: 10 320 residents were enrolled (68.3% female; median age, 38 years); 3105 (30.3%) tested HIV-positive (87.4% on ART) and 1091 (10.6%) reported ≥1 TB symptom. Of 58/10 320 (0.6% [95% CI, .4-.7]) with Mtb culture-positive sputum, 45 (77.6%) reported no symptoms. In both surveys, sputum culture positivity was associated with male sex and reporting >1 TB symptom.
Conclusions: In both clinic and community settings, most participants with Mtb culture-positive sputum were asymptomatic. TB screening based only on symptoms will miss many people with active disease in both settings.
Keywords: South Africa; culture-positive; prevalence; sputum; tuberculosis.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. I. G. reports salary support from the UK Economic and Social Research Council (grant awarded to the London School of Hygiene and Tropical Medicine [LSHTM]). A. S. K. reports support from The Bloomsbury SET (Research England) (grant awarded to their institution, London School of Hygiene & Tropical Medicine), the National Institute for Health Research (UK), Colt Foundation (UK), ViiV Healthcare (USA), Queen Margaret University (UK), World Health Organization, Medical Research Council (UK), London School of Hygiene and Tropical Medicine (UK), and grants awarded to their employer/institution; reports consulting fees from the University of Cape Town (South Africa), South African National TB Think Tank (funded by the Bill and Melinda Gates Foundation, USA), Center for Health Policy and Studies (Republic of Moldova), Vital Strategies (Singapore; funded by Bloomberg Philanthropies, USA), The Aurum Institute (South Africa), and Edanz Group (Japan); reports travel and accommodation costs from Africa Health Research Institute (South Africa), Kyoto University (Japan), University College London (UK), Vital Strategies (Singapore), and Open Access publishing costs from the Bill and Melinda Gates Foundation (USA). K. K. reports salary support and travel expenses and support towards article-processing charges received for a role on the Umoya Omuhle project (from which the paper draws its data) from the UK Economic and Social Research Council (payments made to Queen Margaret University), grant received from the Joint Health Systems Research Initiative (Medical Research Council/Economic and Social Research Council/Department for International Development/Wellcome Trust) and a grant received from the National Institute for Health Research (NIHR; payments made to Queen Margaret University). O. K. reports salary support through grant to the institutions (Africa Health Research Institute [AHRI] and LSHTM) from Wellcome Trust (core grant 082384/Z/07/Z) and the Bill and Melinda Gates Foundation (OPP1175182). T. N. reports support from Wellcome Trust African Academy of Sciences and the South African National Research Foundation, the Bill and Melinda Gates Foundation and Max Planck Society and reports serving as member of the External Advisory Committee for HIV Vaccine Trials Network. E. B. W. reports support from Massachusetts General Hospital, the Africa Health Research Institute, University of Alabama at Birmingham, Bill and Melinda Gates Foundation, Wellcome Trust and National Institutes of Health. A. G. reports funding for other projects paid to their institution by the National Institutes of Allergy and Infectious Diseases, Bill and Melinda Gates Foundation, Research England, Wellcome Trust, and Medical Research Council and reports travel support paid to their institution by Wellcome Trust and Economic and Social Research Council. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Churchyard GJ, Mametja LD, Mvusi L, et al. Tuberculosis control in South Africa: successes, challenges and recommendations. South African Med J 2014; 104:244–8. - PubMed
-
- World Health Organization (WHO). Global tuberculosis report 2020. Geneva, Switzerland: World Health Organization, 2020. Available at: https://www.who.int/publications/i/item/9789240013131. Accessed 22 October 2020.
-
- Loveday M, Mzobe YN, Pillay Y, Barron P, Sa F.. Figures of the dead: a decade of tuberculosis mortality registrations in South Africa. South African Med J 2019; 109:728–32. - PubMed
-
- World Health Organization. Systematic screening for active tuberculosis: principles and recommendations. Geneva, Switzerland: WHO Press, 2013. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
