

Quality of life from cytoreductive surgery in advanced ovarian cancer: Investigating the association between disease burden and surgical complexity in the international, prospective, SOCQER-2 cohort study
- PMID: 34865316
- PMCID: PMC9306902
- DOI: 10.1111/1471-0528.17041
Quality of life from cytoreductive surgery in advanced ovarian cancer: Investigating the association between disease burden and surgical complexity in the international, prospective, SOCQER-2 cohort study
Abstract
Objective: To investigate quality of life (QoL) and association with surgical complexity and disease burden after surgical resection for advanced ovarian cancer in centres with variation in surgical approach.
Design: Prospective multicentre observational study.
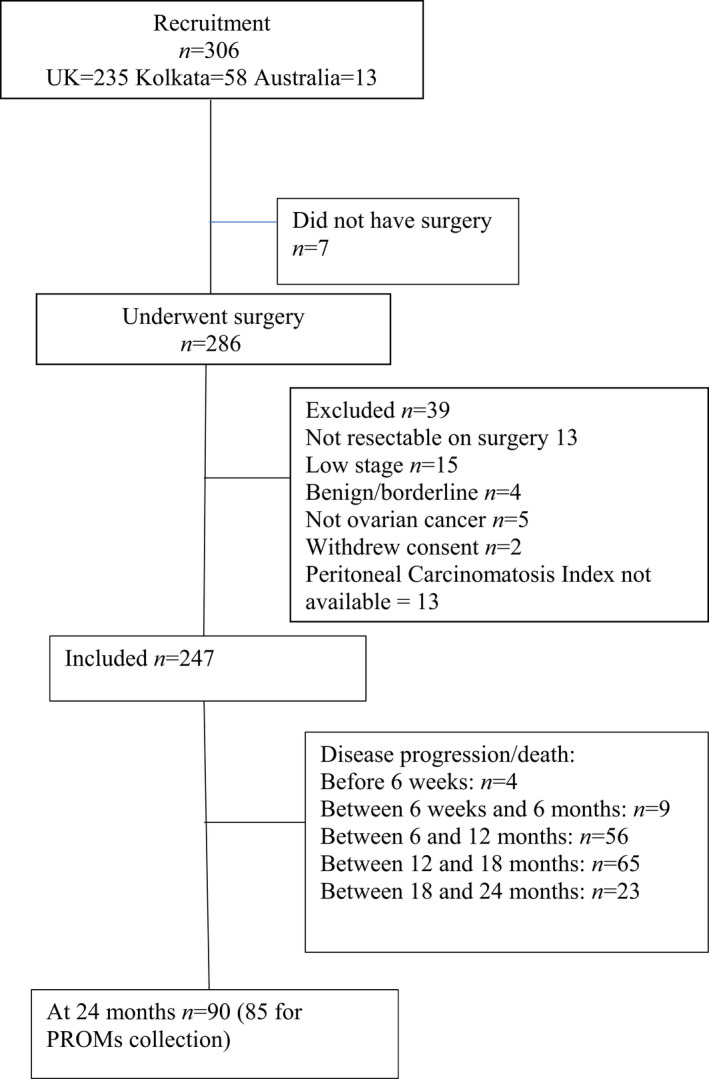
Setting: Gynaecological cancer surgery centres in the UK, Kolkata, India, and Melbourne, Australia.
Sample: Patients undergoing surgical resection (with low, intermediate or high surgical complexity score, SCS) for late-stage ovarian cancer.
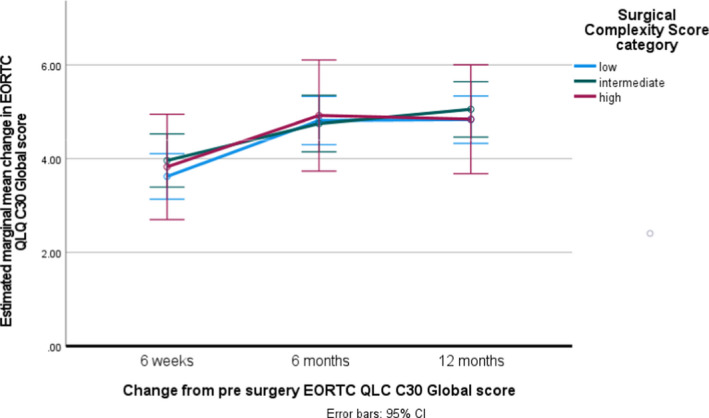
Main outcome measures: Primary: change in global score on the European Organisation for Research and Treatment of Cancer (EORTC) core quality-of-life questionnaire (QLQ-C30). Secondary: EORTC ovarian cancer module (OV28), progression-free survival.
Results: Patients' preoperative disease burden and SCS varied between centres, confirming differences in surgical ethos. QoL response rates were 90% up to 18 months. Mean change from the pre-surgical baseline in the EORTC QLQ-C30 was 3.4 (SD 1.8, n = 88) in the low, 4.0 (SD 2.1, n = 55) in the intermediate and 4.3 (SD 2.1, n = 52) in the high-SCS group after 6 weeks (p = 0.048), and 4.3 (SD 2.1, n = 51), 5.1 (SD 2.2, n = 41) and 5.1 (SD 2.2, n = 35), respectively, after 12 months (p = 0.133). In a repeated-measures model, there were no clinically or statistically meaningful differences in EORTC QLQ-C30 global scores between the three SCS groups (p = 0.840), but there was a small statistically significant improvement in all groups over time (p < 0.001). The high-SCS group experienced small to moderate decreases in physical (p = 0.004), role (p = 0.016) and emotional (p = 0.001) function at 6 weeks post-surgery, which resolved by 6-12 months.
Conclusions: The global QoL of patients undergoing low-, intermediate- and high-SCS surgery improved at 12 months after surgery and was no worse in patients undergoing extensive surgery.
Tweetable abstract: Compared with surgery of lower complexity, extensive surgery does not result in poorer quality of life in patients with advanced ovarian cancer.
Keywords: extensive surgery; ovarian cancer; quality of life; ultraradical surgery.
© 2021 The Authors. BJOG: An International Journal of Obstetrics and Gynaecology published by John Wiley & Sons Ltd.
Conflict of interest statement
SS has received honoraria from Astra Zeneca, MSD and GSK outside the submitted work. CF has received honoraria from Ethicon, Tesaro, MSD/Astra Zeneca, Clovis, Roche, GSK. RM reports grants from Barts Charity, grants from The Eve Appeal, personal fees from Astra Zeneca, MSD, outside the submitted work. RE reports personal fees from Astra Zeneca, personal fees from Clovis Pharma, personal fees from GSK, outside the submitted work. Completed disclosure of interests form available to view online as supporting information. AM reports royalty from Newcastle University (Clovis Oncology) related to the work of development of rucaparib. This is unrelated to the submitted work.
Figures
References
-
- Ozols RF, Bundy BN, Greer BE, Fowler JM, Clarke‐Pearson D, Burger RA, et al. Phase III trial of carboplatin and paclitaxel compared with cisplatin and paclitaxel in patients with optimally resected stage III ovarian cancer: a Gynecologic Oncology Group study. J Clin Oncol. 2003;21(17):3194–200. - PubMed
-
- Jayson GC, Kohn EC, Kitchener HC, Ledermann JA. Ovarian cancer. Lancet. 2014;384(9951):1376–88. - PubMed
-
- Clamp AR, James EC, McNeish IA, Dean A, Kim J‐W, O'Donnell DM, et al. Weekly dose‐dense chemotherapy in first‐line epithelial ovarian, fallopian tube, or primary peritoneal carcinoma treatment (ICON8): primary progression free survival analysis results from a GCIG phase 3 randomised controlled trial. Lancet. 2019;394(10214):2084–95. - PMC - PubMed
-
- Stuart GC, Kitchener H, Bacon M, duBois A, Friedlander M, Ledermann J, et al. 2010 Gynecologic Cancer InterGroup (GCIG) consensus statement on clinical trials in ovarian cancer: report from the Fourth Ovarian Cancer Consensus Conference. Int J Gynecol Cancer. 2011;21(4):750–5. - PubMed
-
- Chi DS, Eisenhauer EL, Zivanovic O, Sonoda Y, Abu‐Rustum NR, Levine DA, et al. Improved progression‐free and overall survival in advanced ovarian cancer as a result of a change in surgical paradigm. Gynecol Oncol. 2009;114(1):26–31. - PubMed
