

Prevalence and impact of airway diseases on clinical outcomes in idiopathic pulmonary fibrosis
- PMID: 34865413
- PMCID: PMC8925941
- DOI: 10.3904/kjim.2021.025
Prevalence and impact of airway diseases on clinical outcomes in idiopathic pulmonary fibrosis
Abstract
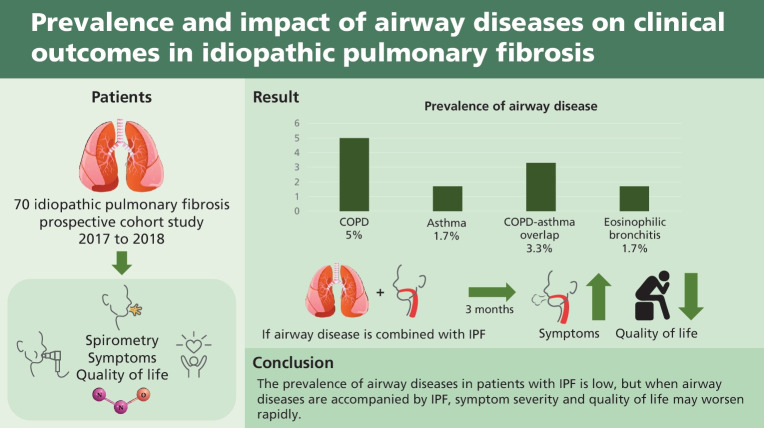
Background/aims: The prevalence and effects of airway diseases, including asthma, eosinophilic bronchitis (EB), chronic obstructive pulmonary disease (COPD), and asthma-COPD overlap (ACO) have not been thoroughly studied in patients with idiopathic pulmonary fibrosis (IPF). This study aimed to evaluate the prevalence of airway diseases in patients with IPF and to identify the differences in symptoms based on the presence of airway diseases.
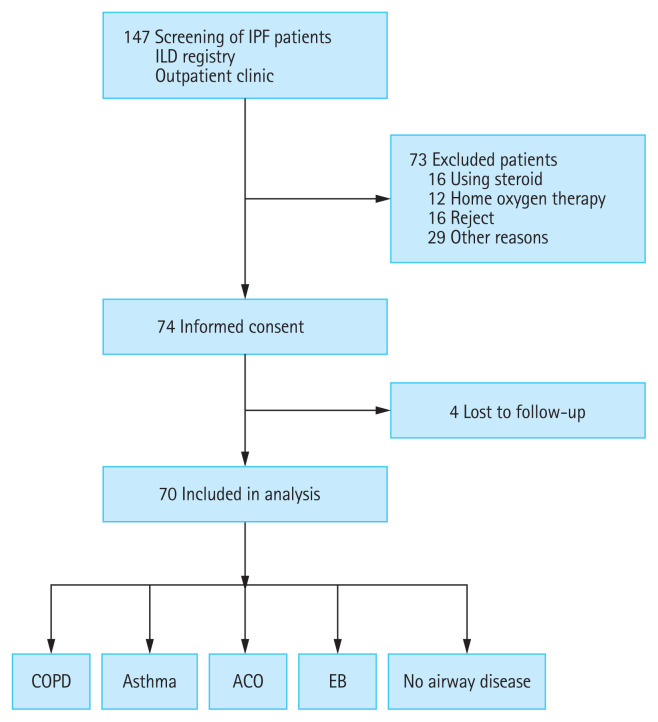
Methods: This single-institution prospective cohort study was conducted from June 2017 to September 2018, at the Seoul National University Hospital. Spirometry with bronchodilator, methacholine bronchial provocation test, induced sputum with eosinophil stain, and exhaled nitric oxide were performed to confirm the presence of airway disease. The modified Medical Research Council (mMRC) dyspnea scale, COPD assessment test (CAT), St. George's Respiratory Questionnaire (SGRQ), EuroQol-5 dimension (EQ-5D) index, and cough-specific quality of life questionnaire (CQLQ) data were collected to assess symptom severity.
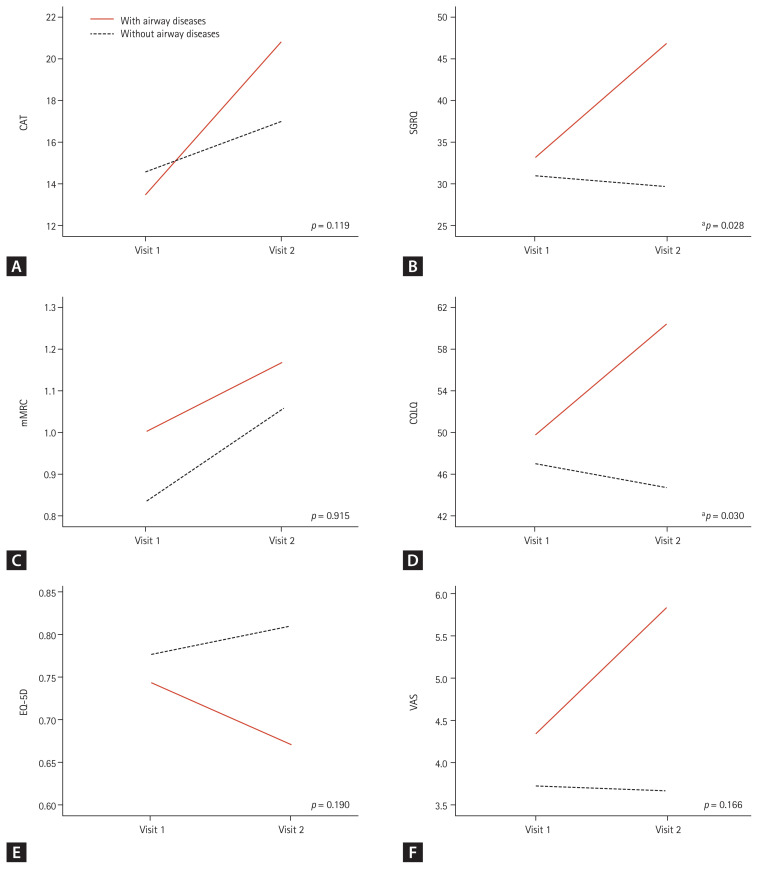
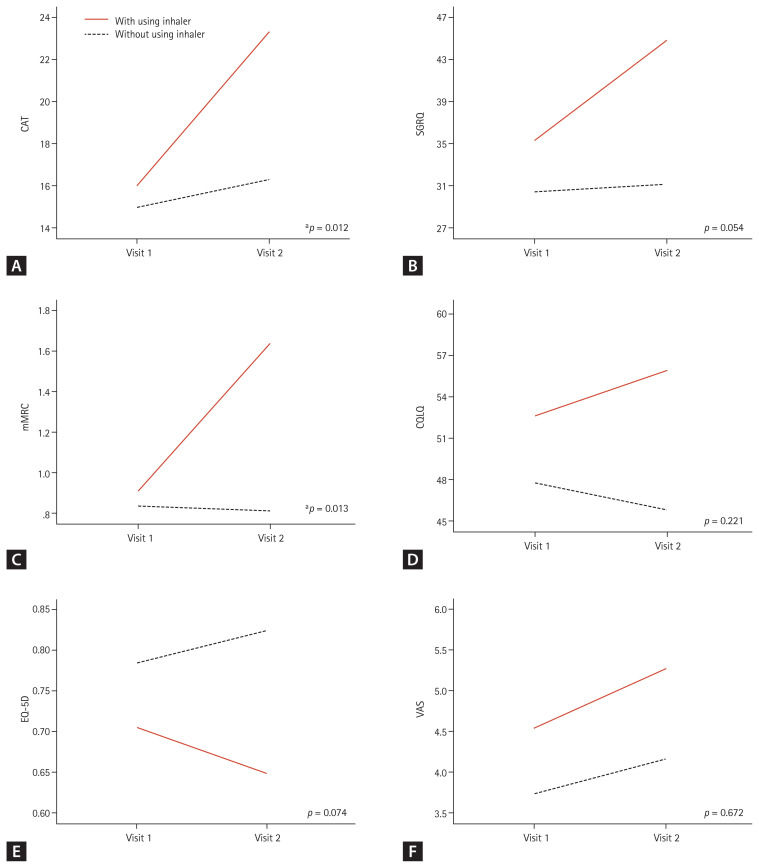
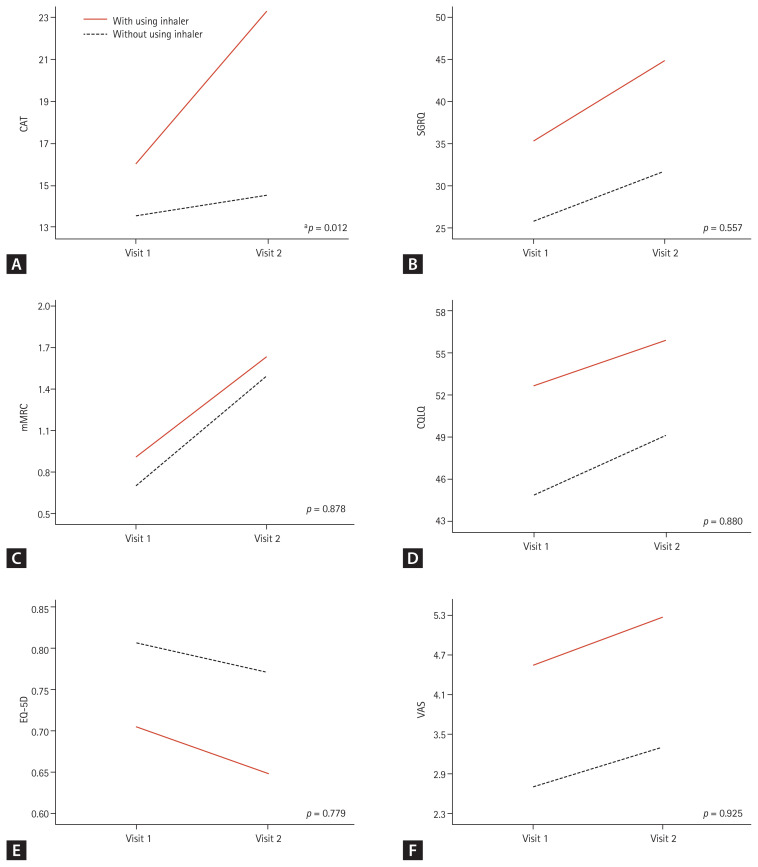
Results: Total 147 patients with IPF were screened, and 70 patients were analyzed. The prevalence of airway diseases in the participants was as follows: 5.0% had COPD, 1.7% had asthma, 3.3% had ACO, and 1.7% had EB. The mMRC, CAT, SGRQ, EQ-5D, and CQLQ scores did not differ regardless of combined airway disease. After 3 months, the SGRQ (p = 0.028) and CQLQ (p = 0.030) scores were significantly higher in patients with airway disease than in those without.
Conclusion: The prevalence of airway diseases in patients with IPF is low, but when airway diseases are accompanied by IPF, symptom severity and quality of life may worsen rapidly.
Keywords: Asthma; Asthma-chronic obstructive pulmonary disease overlap syndrome; Idiopathic pulmonary fibrosis; Pulmonary disease, chronic obstructive; Respiratory therapy.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Raghu G, Rochwerg B, Zhang Y, et al. An official ATS/ERS/JRS/ALAT clinical practice guideline: treatment of idiopathic pulmonary fibrosis. An update of the 2011 Clinical Practice Guideline. Am J Respir Crit Care Med. 2015;192:e3–e19. - PubMed
-
- Crystal RG, Fulmer JD, Roberts WC, Moss ML, Line BR, Reynolds HY. Idiopathic pulmonary fibrosis. Clinical, histologic, radiographic, physiologic, scintigraphic, cytologic, and biochemical aspects. Ann Intern Med. 1976;85:769–788. - PubMed
-
- Shorr AF, Wainright JL, Cors CS, Lettieri CJ, Nathan SD. Pulmonary hypertension in patients with pulmonary fibrosis awaiting lung transplant. Eur Respir J. 2007;30:715–721. - PubMed
-
- Ryerson CJ, Hartman T, Elicker BM, et al. Clinical features and outcomes in combined pulmonary fibrosis and emphysema in idiopathic pulmonary fibrosis. Chest. 2013;144:234–240. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous