

Impact of the COVID-19 pandemic on diagnosis of new cancers: A national multicenter study of the Veterans Affairs Healthcare System
- PMID: 34866184
- PMCID: PMC8837676
- DOI: 10.1002/cncr.34011
Impact of the COVID-19 pandemic on diagnosis of new cancers: A national multicenter study of the Veterans Affairs Healthcare System
Abstract
Background: The coronavirus disease 2019 (COVID-19) pandemic caused disruptions in treatment for cancer. Less is known about its impact on new cancer diagnoses, where delays could cause worsening long-term outcomes. This study quantifies decreases in encounters related to prostate, lung, bladder and colorectal cancers, procedures that facilitate their diagnosis, and new diagnoses of those cancers in the COVID era compared to pre-COVID era.
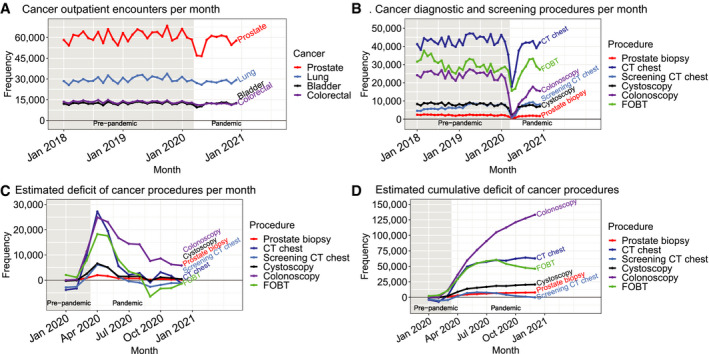
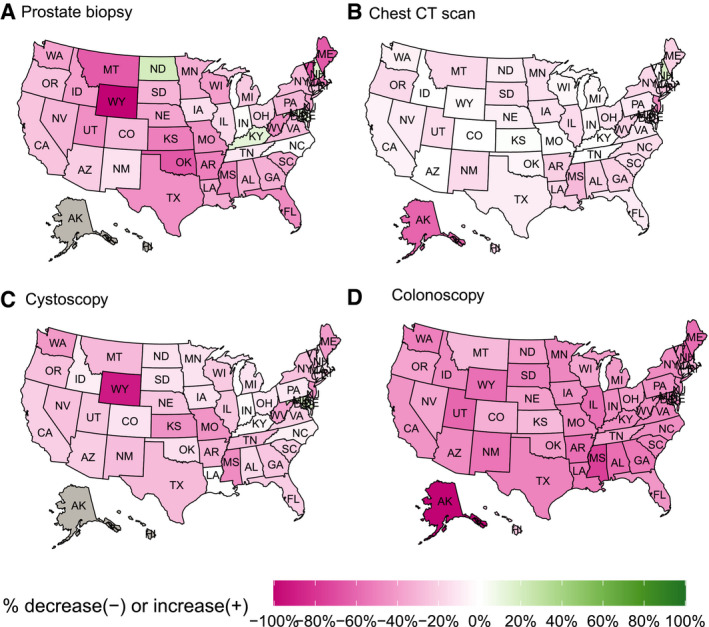
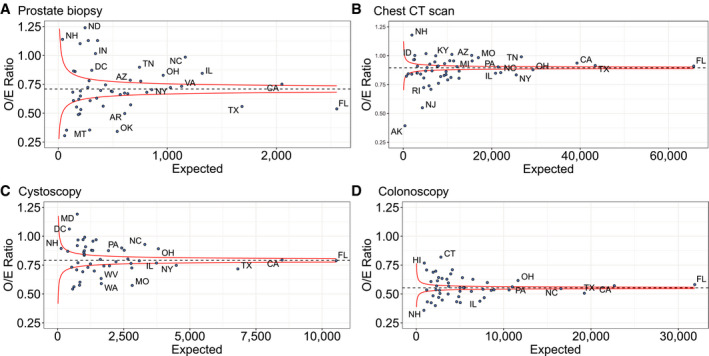
Methods: All encounters at Veterans' Affairs facilities nationwide from 2016 through 2020 were reviewed. The authors quantified trends in new diagnoses of cancer and in procedures facilitating their diagnosis, from January 1, 2018 onward. Using 2018 to 2019 as baseline, reductions in procedures and new cancer diagnoses in 2020 were estimated. Calculated absolute and percentage differences in annual volume and observed-to-expected volume ratios were calculated. Heat maps and funnel plots of volume changes were generated.
Results: From 2018 through 2020, there were 4.1 million cancer-related encounters, 3.9 million relevant procedures, and 251,647 new cancers diagnosed. Compared to the annual averages in 2018 through 2019, colonoscopies in 2020 decreased by 45% whereas prostate biopsies, chest computed tomography scans, and cystoscopies decreased by 29%, 10%, and 21%, respectively. New cancer diagnoses decreased by 13% to 23%. These drops varied by state and continued to accumulate despite reductions in pandemic-related restrictions.
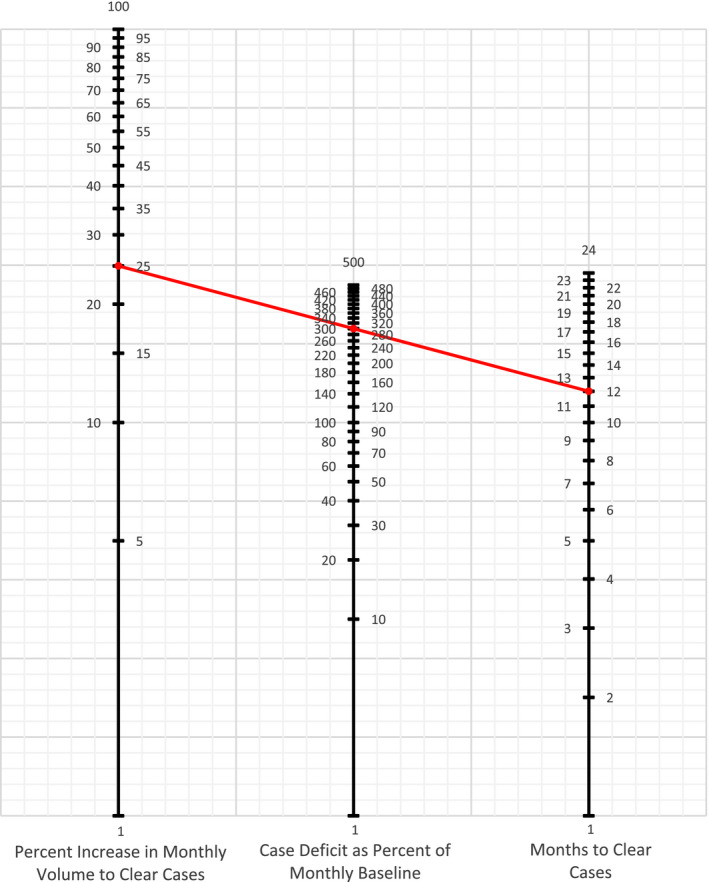
Conclusion: The authors identified substantial reductions in procedures used to diagnose cancer and subsequent reductions in new diagnoses of cancer across the United States because of the COVID-19 pandemic. A nomogram is provided to identify and resolve these unmet health care needs and avoid worse long-term cancer outcomes.
Lay summary: The disruptions due to the COVID-19 pandemic have led to substantial reductions in new cancers being diagnosed. This study quantifies those reductions in a national health care system and offers a method for understanding the backlog of cases and the resources needed to resolve them.
Keywords: bladder cancer; cancer diagnosis; cancer screening; colorectal cancer; coronavirus disease 2019 (COVID-19); lung cancer; prostate cancer.
© 2021 American Cancer Society.
Conflict of interest statement
Brajesh K. Lal received grants from the Department of Veterans Affairs (RRD RX000995 and CSRD CX001621) and the National Institutes of Health (NS080168, NS097876, and AG000513). John D. Sorkin received grants from the National Institutes of Health (AG028747 and DK072488) and the Baltimore VA Medical Centre GRECC. Nikhil K. Prasad received a grant from the National Institutes of Health (T32 AG00262). The other authors made no disclosures.
Figures

Comment in
-
Study of the Veterans Affairs Health Care System highlights the impact of COVID-19 on cancer diagnoses in the USA.Lancet Oncol. 2022 Jan;23(1):21. doi: 10.1016/S1470-2045(21)00713-0. Epub 2021 Dec 13. Lancet Oncol. 2022. PMID: 34914888 Free PMC article. No abstract available.
-
Reply to "Cancer treatment in the time of COVID-19 pandemics: A new concern".Cancer. 2022 Aug 1;128(15):2992-2993. doi: 10.1002/cncr.34250. Epub 2022 May 2. Cancer. 2022. PMID: 35499669 Free PMC article. No abstract available.
-
Cancer treatment in the time of COVID-19 pandemics: A new concern.Cancer. 2022 Aug 1;128(15):2991. doi: 10.1002/cncr.34249. Epub 2022 May 2. Cancer. 2022. PMID: 35499670 Free PMC article. No abstract available.
References
-
- Non‐emergent, elective medical services, and treatment recommendations. Centers for Medicare & Medicaid Services. Accessed September 17, 2020. https://www.cms.gov/files/document/cms‐non‐emergent‐elective‐medical‐rec...
-
- COVID‐19: guidance for triage of non‐emergent surgical procedures. American College of Surgeons. Accessed October 8, 2020. https://www.facs.org/COVID‐19/clinical‐guidance/triage
-
- COVID Response Team, New York City Department of Health and Mental Hygiene . Preliminary estimate of excess mortality during the COVID‐19 outbreak‐New York City, March 11‐May 2, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:603‐605. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
