

Effects of Sodium-Glucose Transporter 2 Inhibitors (SGLT2-I) in Patients With Ischemic Heart Disease (IHD) Treated by Coronary Artery Bypass Grafting via MiECC: Inflammatory Burden, and Clinical Outcomes at 5 Years of Follow-Up
- PMID: 34867407
- PMCID: PMC8634684
- DOI: 10.3389/fphar.2021.777083
Effects of Sodium-Glucose Transporter 2 Inhibitors (SGLT2-I) in Patients With Ischemic Heart Disease (IHD) Treated by Coronary Artery Bypass Grafting via MiECC: Inflammatory Burden, and Clinical Outcomes at 5 Years of Follow-Up
Abstract
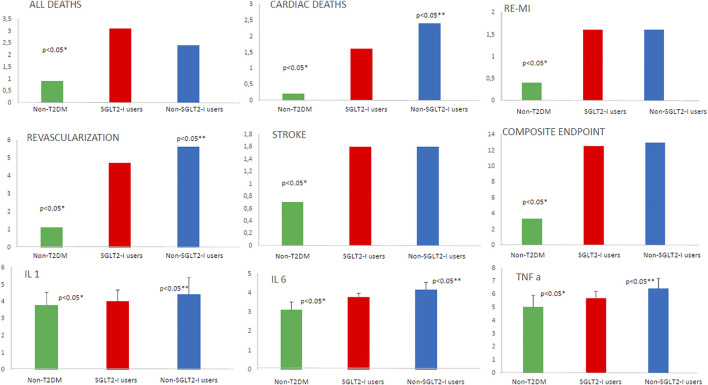
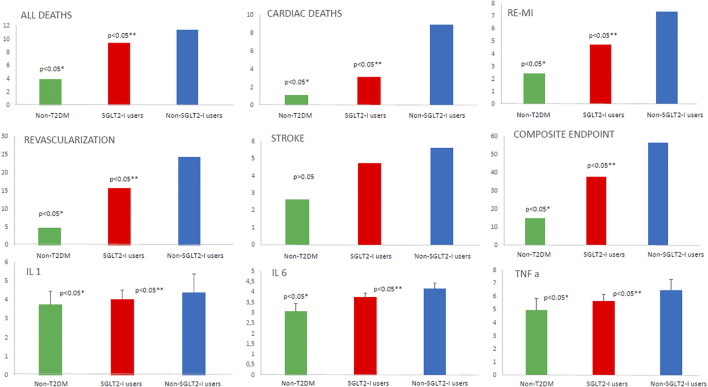
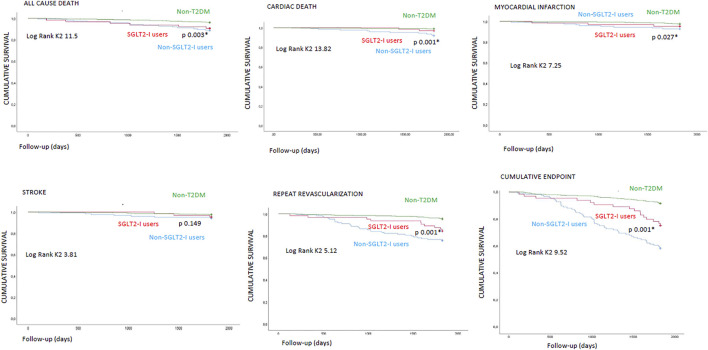
Introduction: Minimally invasive extracorporeal circulation (MiECC) reduced inflammatory burden, leading to best clinical outcomes in patients treated with coronary artery bypass grafting (CABG). Despite this, the patients with type 2 diabetes mellitus (T2DM) vs those without T2DM (non-T2DM) have a worse prognosis, caused by over-inflammation and modulated by sodium-glucose transporter 2 receptors. However, we evaluated the inflammatory burden and clinical outcomes in non-T2DM vs T2DM patients under sodium-glucose transporter 2 inhibitors (SGLT2-I users) vs non-SGLT2-I users at 5 years of follow-up post-CABG via MiECC. Materials and methods: In a multicenter study, we screened consecutive patients with indications to receive CABG. The study endpoints were the inflammatory burden (circulating serum levels of tumor necrosis factor-alpha (TNF-α), interleukin 1 and 6 (IL-1 and IL-6), C-reactive protein (CRP), and leucocytes count) and the clinical outcomes at follow-up of 5 years in non-T2DM vs SGLT2-I users, in non-T2DM vs non-SGLT2-I users, and SGLT2-I users vs non-SGLT2-I users. Results: At baseline, and at one year and 5 years of follow-up, the non-T2DM vs SGLT2-I users, non-T2DM vs non-SGLT2-I users, and SGLT2-I users vs non-SGLT2-I users had the lowest values of IL-1, IL-6, and TNF-α (p < 0.05). At one year of follow-up, SGLT2-I users vs non-T2DM and non-SGLT2-I users vs non-T2DM users had a higher rate of all deaths, cardiac deaths, re-myocardial infarction, repeat revascularization, and stroke, and of the composite endpoint (p < 0.05). In a multivariate Cox regression analysis, the composite endpoint was predicted by IL-1 [2.068 (1.367-3.129)], TNF-α [1.989 (1.081-2.998)], and SGLT2-I [0.504 (0.078-0.861)]. Conclusion: In T2DM patients, the SGLT2-I significantly reduced the inflammatory burden and ameliorated clinical outcomes at 5 years of follow-up post-CABG via MiECC.
Keywords: coronary artery bypass grafting; minimally invasive extracorporeal circulation; multi-vessel coronary stenosis; over-inflammation; sodium-glucose transporter 2 inhibitors; type 2 diabetes mellitus, coronary heart disease.
Copyright © 2021 Sardu, Massetti, Testa, Martino, Castellano, Turriziani, Sasso, Torella, De Feo, Santulli, Paolisso and Marfella.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Anastasiadis K., Murkin J., Antonitsis P., Bauer A., Ranucci M., Gygax E., et al. (2016). Use of Minimal Invasive Extracorporeal Circulation in Cardiac Surgery: Principles, Definitions and Potential Benefits. A Position Paper from the Minimal Invasive Extra-corporeal Technologies International Society (MiECTiS). Interact Cardiovasc. Thorac. Surg. 22 (5), 647–662. 10.1093/icvts/ivv380 - DOI - PMC - PubMed
-
- D'Onofrio N., Sardu C., Trotta M. C., Scisciola L., Turriziani F., Ferraraccio F., et al. (2021). Sodium-glucose Co-transporter2 Expression and Inflammatory Activity in Diabetic Atherosclerotic Plaques: Effects of Sodium-Glucose Co-transporter2 Inhibitor Treatment. Mol. Metab. 54, 101337. 10.1016/j.molmet.2021.101337 - DOI - PMC - PubMed
-
- Gallinoro E., Paolisso P., Candreva A., Bermpeis K., Fabbricatore D., Esposito G., et al. (2021). Microvascular Dysfunction in Patients with Type II Diabetes Mellitus: Invasive Assessment of Absolute Coronary Blood Flow and Microvascular Resistance Reserve. Front. Cardiovasc. Med., 8. 10.3389/fcvm.2021.765071 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous