

Malaria in Pregnancy: From Placental Infection to Its Abnormal Development and Damage
- PMID: 34867919
- PMCID: PMC8636035
- DOI: 10.3389/fmicb.2021.777343
Malaria in Pregnancy: From Placental Infection to Its Abnormal Development and Damage
Abstract
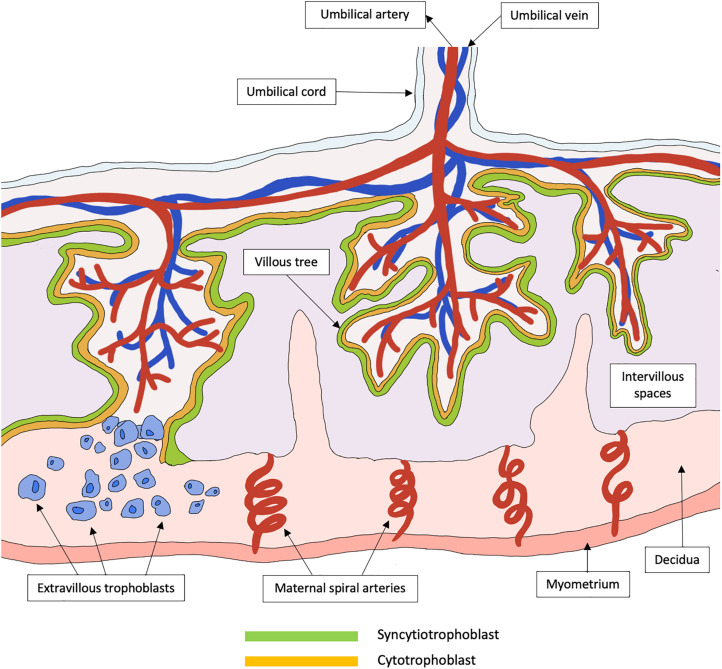
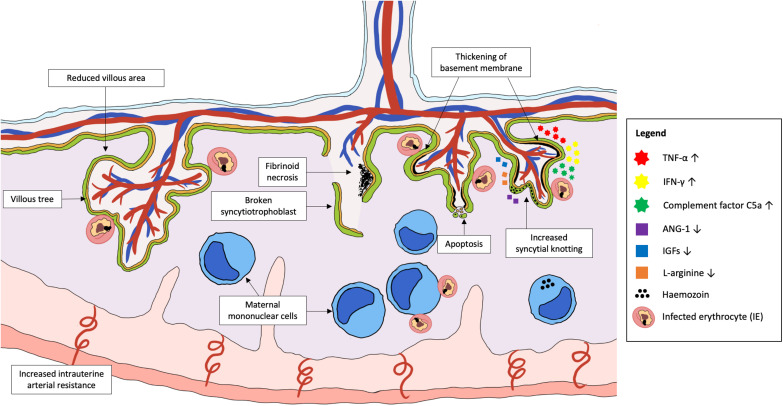
Malaria remains a global health burden with Plasmodium falciparum accounting for the highest mortality and morbidity. Malaria in pregnancy can lead to the development of placental malaria, where P. falciparum-infected erythrocytes adhere to placental receptors, triggering placental inflammation and subsequent damage, causing harm to both mother and her infant. Histopathological studies of P. falciparum-infected placentas revealed various placental abnormalities such as excessive perivillous fibrinoid deposits, breakdown of syncytiotrophoblast integrity, trophoblast basal lamina thickening, increased syncytial knotting, and accumulation of mononuclear immune cells within intervillous spaces. These events in turn, are likely to impair placental development and function, ultimately causing placental insufficiency, intrauterine growth restriction, preterm delivery and low birth weight. Hence, a better understanding of the mechanisms behind placental alterations and damage during placental malaria is needed for the design of effective interventions. In this review, using evidence from human studies and murine models, an integrated view on the potential mechanisms underlying placental pathologies in malaria in pregnancy is provided. The molecular, immunological and metabolic changes in infected placentas that reflect their responses to the parasitic infection and injury are discussed. Finally, potential models that can be used by researchers to improve our understanding on the pathogenesis of malaria in pregnancy and placental pathologies are presented.
Keywords: Plasmodium falciparum; fetal growth restriction; low birth weight; malaria; placental insufficiency; pregnancy; preterm birth; syncytiotrophoblast.
Copyright © 2021 Chua, Khoo, Ong, Ramireddi, Yeo and Teo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources