

Immune Dysregulation in Patients With Chromosome 18q Deletions-Searching for Putative Loci for Autoimmunity and Immunodeficiency
- PMID: 34867966
- PMCID: PMC8637865
- DOI: 10.3389/fimmu.2021.742834
Immune Dysregulation in Patients With Chromosome 18q Deletions-Searching for Putative Loci for Autoimmunity and Immunodeficiency
Abstract
Introduction: Autoimmune disorders, IgA deficiency, and allergies seem to be common among individuals with 18q deletion syndrome [OMIM 601808]. We aimed to determine the prevalence, mechanism, and genetic background of autoimmunity, immune deficiency, and allergy in a cohort of patients with 18q deletions.
Material and methods: Medical registries and social media were used to recruit the patients. Microarray oligonucleotide comparative genomic hybridization (aCGH) (Agilent, Santa Clara, CA, USA) was performed in all patients to identify size and location of chromosome 18 deletion. Clinical evaluation and medical record collection were performed in each of the study participants. The history of autoimmune disorders, severe and/or recurrent infections, and symptoms of allergy were noted. Total immunoglobulin IgG, IgA, IgM, IgE, and IgG1-4 serum levels were measured using nephelometry and ELISA methods. Lymphocyte T subset phenotyping was performed in 24 subjects from 18q del cohort. To predict the most promising candidate genes, we used the ENDEAVOUR-a free web resource for gene prioritization.
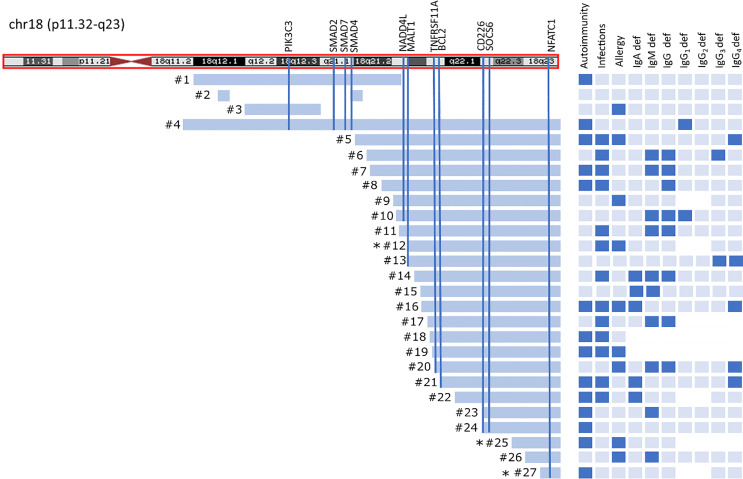
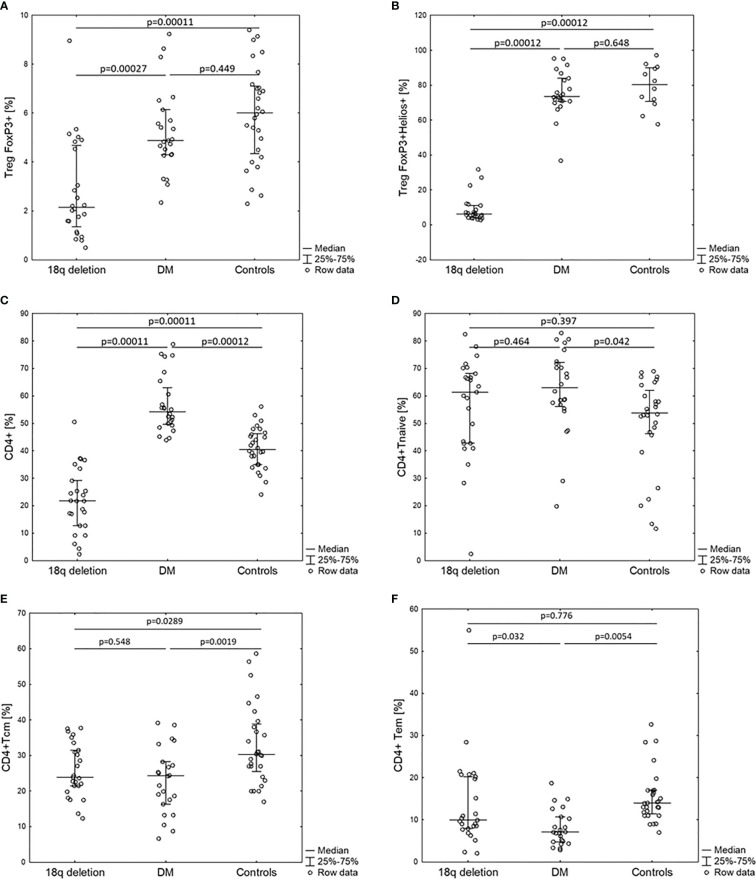
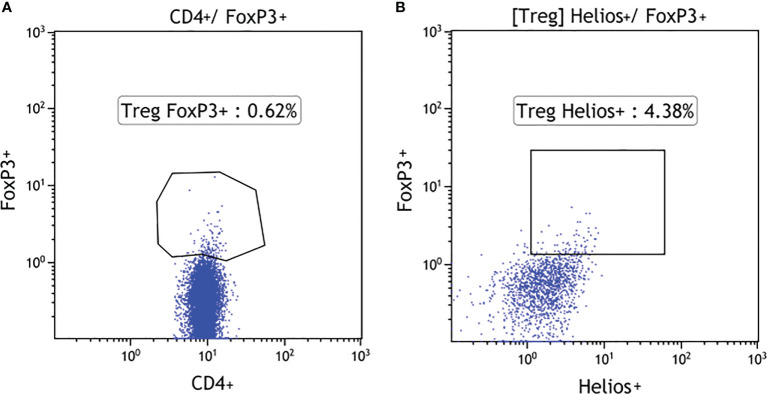
Results: 18q deletion was confirmed by means of array CGH analysis in 27 individuals, 15 (55.6%) females and 12 males, referred to the project by specialists in medical genetics, diabetology, or pediatric endocrinology between May 2015 and December 2019. The mean age at examination was 11.8 years (min-max: 4.0-33.5). Autoimmune disorders were present in 14/27 (51.8%) of the cohort. In eight of patients, symptoms of immune deficiency coexisted with autoimmunity. Allergy was reported in nine of 27 (33.4%) patients. Over 89% of patients presented with at list one type of immunoglobulin (IgA, IgM, IgG, IgE, and IgG1-4) deficiency and eight of 25 (32%) had abnormalities in at least two major immunoglobulin (IgG, IgA, IgM) measurements (CVID-like phenotype). Patients with 18q del exhibited a significantly decreased CD4, Treg FOXP3+, TregFOXP3+Helios+, and TemCD4 cell numbers in comparison with the control groups of 24 T1DM patients and 28 healthy controls.
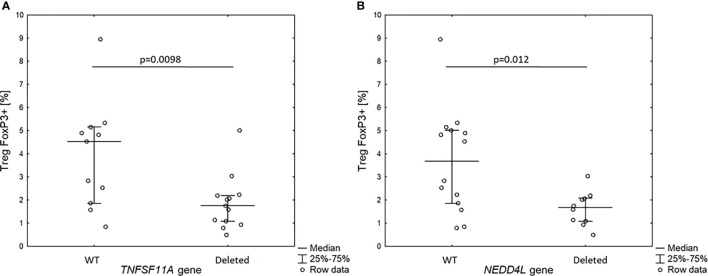
Conclusions: Patients with 18q deletions frequently suffer from autoimmune disorders, recurrent infections, and allergy due to immune dysregulation presenting with variable antibody deficiencies and T-regulatory cell deficiency (CD4+CD25+CD127lowFOXP3+). The spectrum of speculations regarding which gene might be responsible for such phenotype ranges from single gene haploinsufficiency to deletion of a cluster of immunogenes located distally to 18q21.
Keywords: 18q deletion syndrome; T regulatory cells; antibody deficiency; autoimmune diseases; immune deficiency; thyroiditis; type 1 diabetes.
Copyright © 2021 Hogendorf, Zieliński, Constantinou, Śmigiel, Wierzba, Wyka, Wędrychowicz, Jakubiuk-Tomaszuk, Budzynska, Piotrowicz, Lipska-Ziętkiewicz, Kaczorowska, Cieślikowska, Kutkowska-Kaźmierczak, Fijak-Moskal, Kugaudo, Kosińska-Urbańska, Szadkowska, Borowiec, Niedźwiecki, Trzonkowski and Młynarski.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous