

Evaluation of Critical Factors of Postoperative Arrhythmia and Preventive Measures of Deep Venous Thrombosis
- PMID: 34868315
- PMCID: PMC8635950
- DOI: 10.1155/2021/6103092
Evaluation of Critical Factors of Postoperative Arrhythmia and Preventive Measures of Deep Venous Thrombosis
Retraction in
-
Retracted: Evaluation of Critical Factors of Postoperative Arrhythmia and Preventive Measures of Deep Venous Thrombosis.J Oncol. 2023 Aug 2;2023:9854354. doi: 10.1155/2023/9854354. eCollection 2023. J Oncol. 2023. PMID: 37564264 Free PMC article.
Abstract
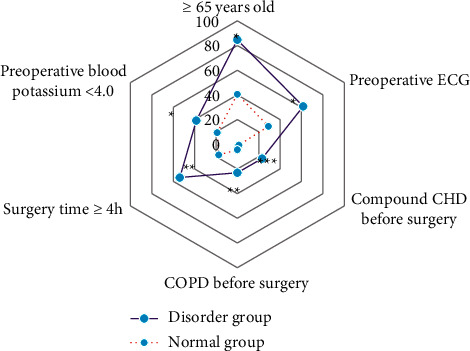
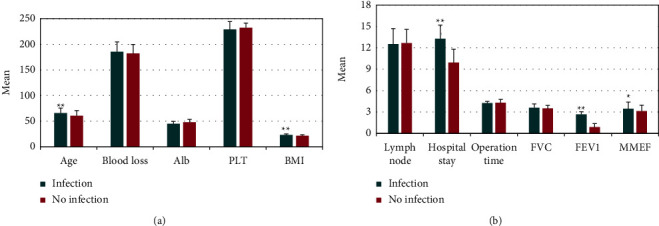
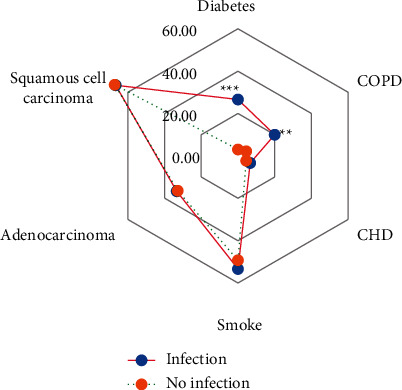
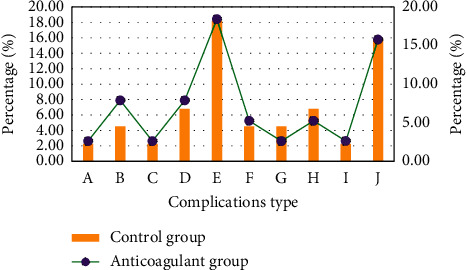
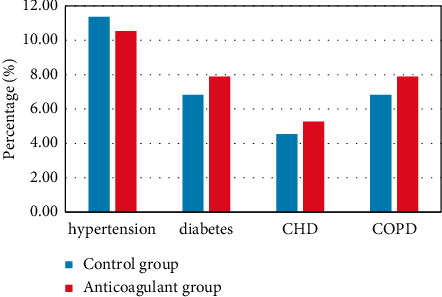
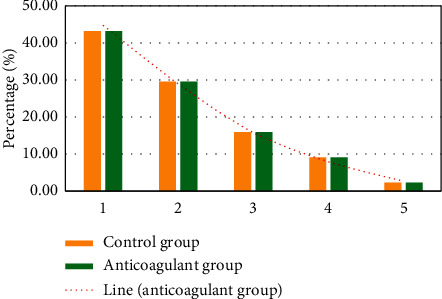
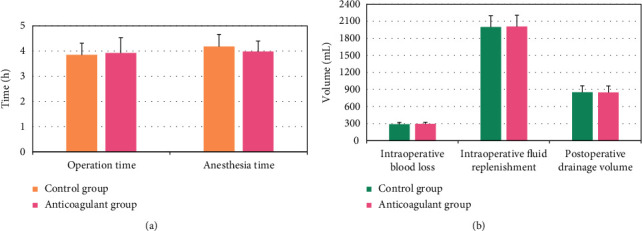
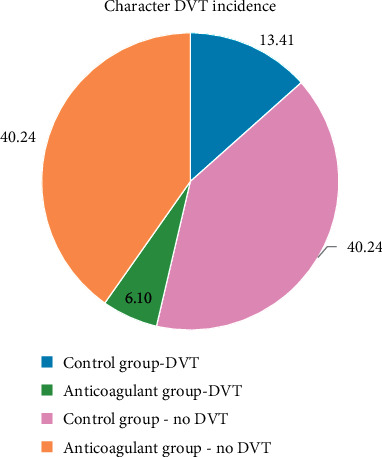
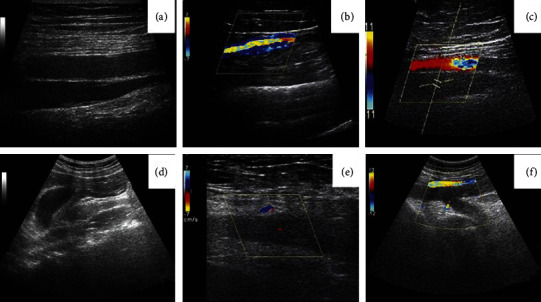
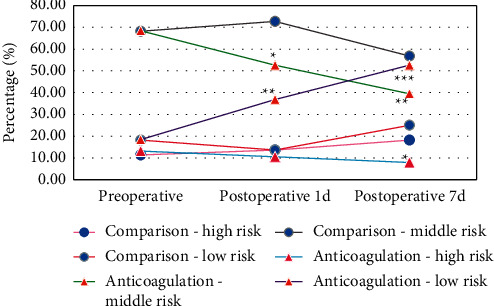
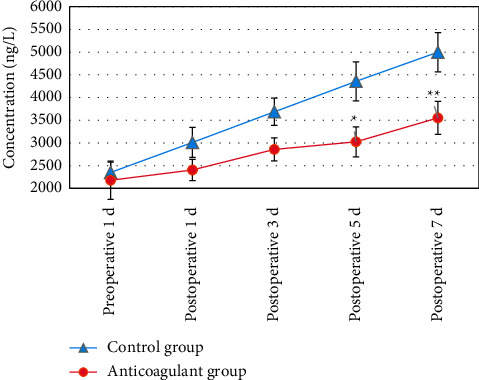
The study focused on the risk factors of postoperative arrhythmia and lung infection and the preventive effects of targeted low-molecular-weight heparin (LMWH) on the occurrence of deep venous thrombosis (DVT) in patients with esophageal/cardia cancer. In this article, 82 patients who were pathologically diagnosed with esophageal/cardia cancer and underwent surgical treatment were selected as the research subjects. According to the different preoperative treatment methods, the patients were divided into the control group (without anticoagulant drugs before the operation, 44 cases) and the anticoagulation group (anticoagulant drugs were administered before the operation, 38 cases), and they were compared for basic clinical indicators and disease history. Logistic regression analysis was performed to analyze the risk factors of adverse events, and the Wells and Autar scale scores were calculated. Different groups were compared for the operation time, blood loss, and postoperative drainage volume during the operation. D-dimer was detected on the first 1, 3, 5, and 7 days after the operation, and the lower extremity venous color Doppler ultrasound was performed on the 1st and 7th days after the operation. The results showed that age ≥65 years, abnormal preoperative ECG, preoperative coronary heart disease (CHD), preoperative chronic obstructive pulmonary disease (COPD), operative time ≥4 h, and preoperative blood sodium <4.04.0 mmol/L were all risk factors for postoperative arrhythmia. Age, preoperative diabetes mellitus, preoperative COPD, length of hospital stay, and FEV1 were all risk factors for postoperative lung infections. In the control group and anticoagulation group, 11 cases (13.41%) and 5 cases (16.10%) had lower extremity DVT, respectively. The incidence of lower extremity DVT was lower in the anticoagulation group than in the control group (P < 0.01). It suggested that age, preoperative disease history, hospital stay, and operation time were risk factors for postoperative adverse events in patients with esophageal/cardia cancer. The targeted anticoagulant LMWH has a significant preventive effect on the occurrence of lower extremity DVT in patients with esophageal/cardia cancer, providing an effective reference for the prognosis and prevention of esophageal/cardia cancer.
Copyright © 2021 Boheng Liu et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Incidence of venous thromboembolism and hemorrhage related safety studies of preoperative anticoagulation therapy in hip fracture patients undergoing surgical treatment: a case-control study.BMC Musculoskelet Disord. 2016 Feb 12;17:76. doi: 10.1186/s12891-016-0917-y. BMC Musculoskelet Disord. 2016. PMID: 26873584 Free PMC article.
-
[Risk Factors Associated with Venous Thromboembolism after Lung Cancer Surgery: A Single-center Study].Zhongguo Fei Ai Za Zhi. 2018 Oct 20;21(10):753-760. doi: 10.3779/j.issn.1009-3419.2018.10.04. Zhongguo Fei Ai Za Zhi. 2018. PMID: 30309426 Free PMC article. Chinese.
-
Analysis of perioperative risk factors for deep vein thrombosis in patients with femoral and pelvic fractures.J Orthop Surg Res. 2020 Dec 10;15(1):597. doi: 10.1186/s13018-020-02131-5. J Orthop Surg Res. 2020. PMID: 33302974 Free PMC article.
-
[Clinical features of patients with venous thromboembolism: 177 case analysis in 10 years].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019 Apr;31(4):453-457. doi: 10.3760/cma.j.issn.2095-4352.2019.04.016. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019. PMID: 31109420 Review. Chinese.
-
Interventions for preventing venous thromboembolism in adults undergoing knee arthroscopy.Cochrane Database Syst Rev. 2020 May 6;5(5):CD005259. doi: 10.1002/14651858.CD005259.pub4. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2022 Aug 22;8:CD005259. doi: 10.1002/14651858.CD005259.pub5. PMID: 32374919 Free PMC article. Updated.
Cited by
-
Retracted: Evaluation of Critical Factors of Postoperative Arrhythmia and Preventive Measures of Deep Venous Thrombosis.J Oncol. 2023 Aug 2;2023:9854354. doi: 10.1155/2023/9854354. eCollection 2023. J Oncol. 2023. PMID: 37564264 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
