

The Clinical Significance and Transcription Regulation of a DNA Damage Repair Gene, SMC4, in Low-Grade Glioma via Integrated Bioinformatic Analysis
- PMID: 34868977
- PMCID: PMC8636002
- DOI: 10.3389/fonc.2021.761693
The Clinical Significance and Transcription Regulation of a DNA Damage Repair Gene, SMC4, in Low-Grade Glioma via Integrated Bioinformatic Analysis
Abstract
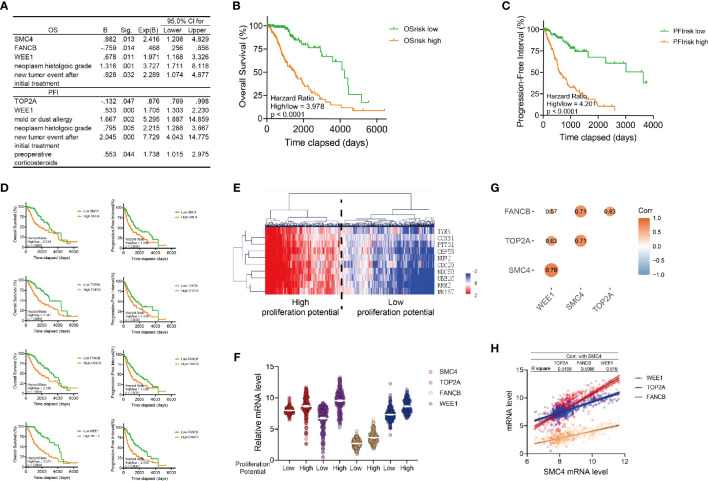
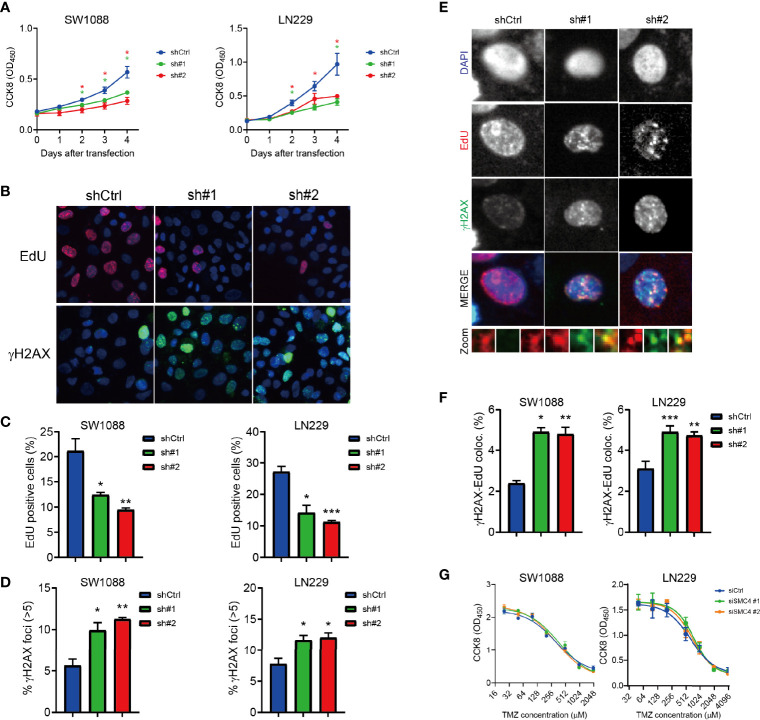
Glioma is the most common type of malignant tumor in the central nervous system with an unfavorable prognosis and limited treatment. In this study, we are devoted to addressing the prognostic value of DNA damage repair-related genes in low-grade glioma (LGG). We plotted the landscape of DNA damage repair (DDR)-related genes and identified SMC4 as an independent prognostic marker with integrated bioinformatics analysis, which is overexpressed in different histologic subtypes of glioma. We observed that SMC4 expression is elevated in recurrent LGG patients or those with advanced histologic staging. SMC4 depletion inhibits proliferation and induces increased replication damage in LGG cells. Lastly, we predicted and validated the transcription modulation of SMC4 by a transcription factor, MYB, at the -976bp~ -837bp of the SMC4 promoter region in LGG cells. Together, our study identified SMC4 as a potential prognostic biomarker for LGG patients, which functions to promote cell proliferation by repairing replication damage and the expression of SMC4 could be transcriptionally regulated by MYB.
Keywords: DNA damage repair; SMC4; bioinformatic; low-grade glioma; transcriptional modulation.
Copyright © 2021 Wang and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




Similar articles
-
SMC4, a novel tumor prognostic marker and potential tumor therapeutic target.Front Oncol. 2023 Mar 17;13:1117642. doi: 10.3389/fonc.2023.1117642. eCollection 2023. Front Oncol. 2023. PMID: 37007153 Free PMC article. Review.
-
Genomic Profiling of Lower-Grade Gliomas Subtype with Distinct Molecular and Clinicopathologic Characteristics via Altered DNA-Damage Repair Features.J Mol Neurosci. 2023 May;73(4-5):269-286. doi: 10.1007/s12031-023-02116-z. Epub 2023 Apr 17. J Mol Neurosci. 2023. PMID: 37067735
-
Serine Incorporator 2 (SERINC2) Expression Predicts an Unfavorable Prognosis of Low-Grade Glioma (LGG): Evidence from Bioinformatics Analysis.J Mol Neurosci. 2020 Oct;70(10):1521-1532. doi: 10.1007/s12031-020-01620-w. Epub 2020 Jul 8. J Mol Neurosci. 2020. PMID: 32642801 Free PMC article.
-
Overexpression of SMC4 activates TGFβ/Smad signaling and promotes aggressive phenotype in glioma cells.Oncogenesis. 2017 Mar 13;6(3):e301. doi: 10.1038/oncsis.2017.8. Oncogenesis. 2017. PMID: 28287612 Free PMC article.
-
Elevated TYROBP expression predicts poor prognosis and high tumor immune infiltration in patients with low-grade glioma.BMC Cancer. 2021 Jun 23;21(1):723. doi: 10.1186/s12885-021-08456-6. BMC Cancer. 2021. PMID: 34162355 Free PMC article.
Cited by
-
FoxO1 promotes ovarian cancer by increasing transcription and METTL14-mediated m6A modification of SMC4.Cancer Sci. 2024 Apr;115(4):1224-1240. doi: 10.1111/cas.16120. Epub 2024 Feb 25. Cancer Sci. 2024. PMID: 38403332 Free PMC article.
-
Correlation between DNA Methylation and Cell Proliferation Identifies New Candidate Predictive Markers in Meningioma.Cancers (Basel). 2022 Dec 17;14(24):6227. doi: 10.3390/cancers14246227. Cancers (Basel). 2022. PMID: 36551712 Free PMC article.
-
SMC4, a novel tumor prognostic marker and potential tumor therapeutic target.Front Oncol. 2023 Mar 17;13:1117642. doi: 10.3389/fonc.2023.1117642. eCollection 2023. Front Oncol. 2023. PMID: 37007153 Free PMC article. Review.
-
A mini-review of the role of condensin in human nervous system diseases.Front Mol Neurosci. 2022 Aug 4;15:889796. doi: 10.3389/fnmol.2022.889796. eCollection 2022. Front Mol Neurosci. 2022. PMID: 35992200 Free PMC article. Review.
-
A metabolic map of the DNA damage response identifies PRDX1 in the control of nuclear ROS scavenging and aspartate availability.Mol Syst Biol. 2023 Jul 11;19(7):e11267. doi: 10.15252/msb.202211267. Epub 2023 Jun 1. Mol Syst Biol. 2023. PMID: 37259925 Free PMC article.
References
LinkOut - more resources
Full Text Sources