

Development and Validation of the 5-SENSE Score to Predict Focality of the Seizure-Onset Zone as Assessed by Stereoelectroencephalography
- PMID: 34870697
- PMCID: PMC8649918
- DOI: 10.1001/jamaneurol.2021.4405
Development and Validation of the 5-SENSE Score to Predict Focality of the Seizure-Onset Zone as Assessed by Stereoelectroencephalography
Abstract
Importance: Stereoelectroencephalography (SEEG) has become the criterion standard in case of inconclusive noninvasive presurgical epilepsy workup. However, up to 40% of patients are subsequently not offered surgery because the seizure-onset zone is less focal than expected or cannot be identified.
Objective: To predict focality of the seizure-onset zone in SEEG, the 5-point 5-SENSE score was developed and validated.
Design, setting, and participants: This was a monocentric cohort study for score development followed by multicenter validation with patient selection intervals between February 2002 to October 2018 and May 2002 to December 2019. The minimum follow-up period was 1 year. Patients with drug-resistant epilepsy undergoing SEEG at the Montreal Neurological Institute were analyzed to identify a focal seizure-onset zone. Selection criteria were 2 or more seizures in electroencephalography and availability of complete neuropsychological and neuroimaging data sets. For validation, patients from 9 epilepsy centers meeting these criteria were included. Analysis took place between May and July 2021.
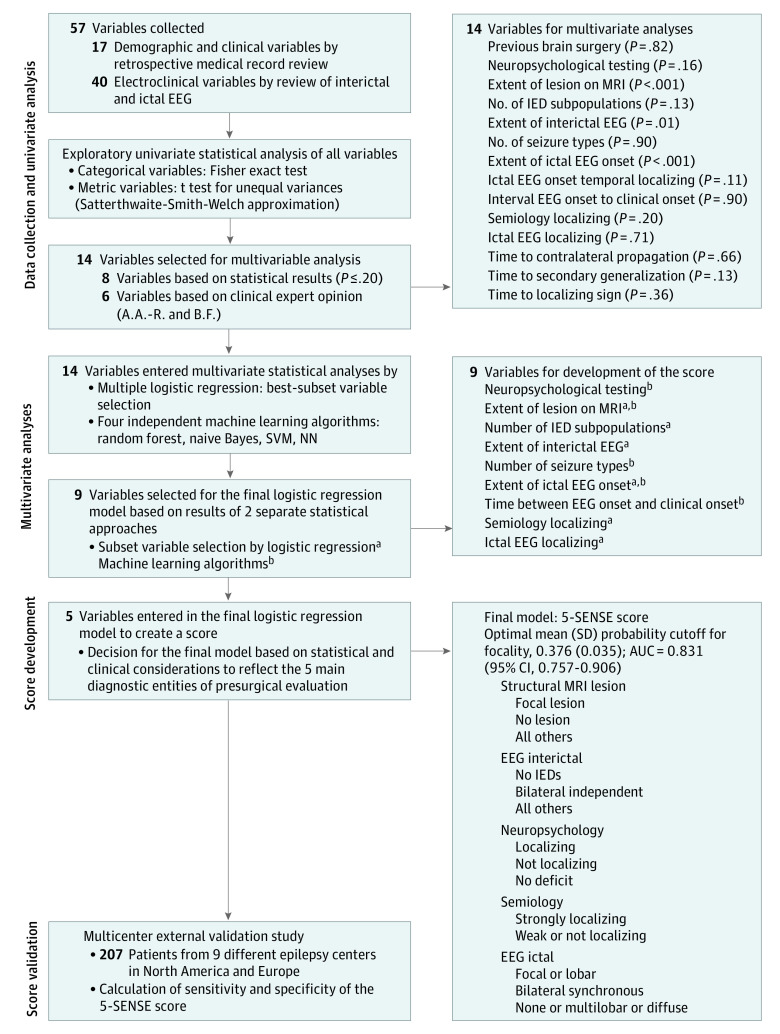
Main outcomes and measures: Based on SEEG, patients were grouped as focal and nonfocal seizure-onset zone. Demographic, clinical, electroencephalography, neuroimaging, and neuropsychology data were analyzed, and a multiple logistic regression model for developing a score to predict SEEG focality was created and validated in an independent sample.
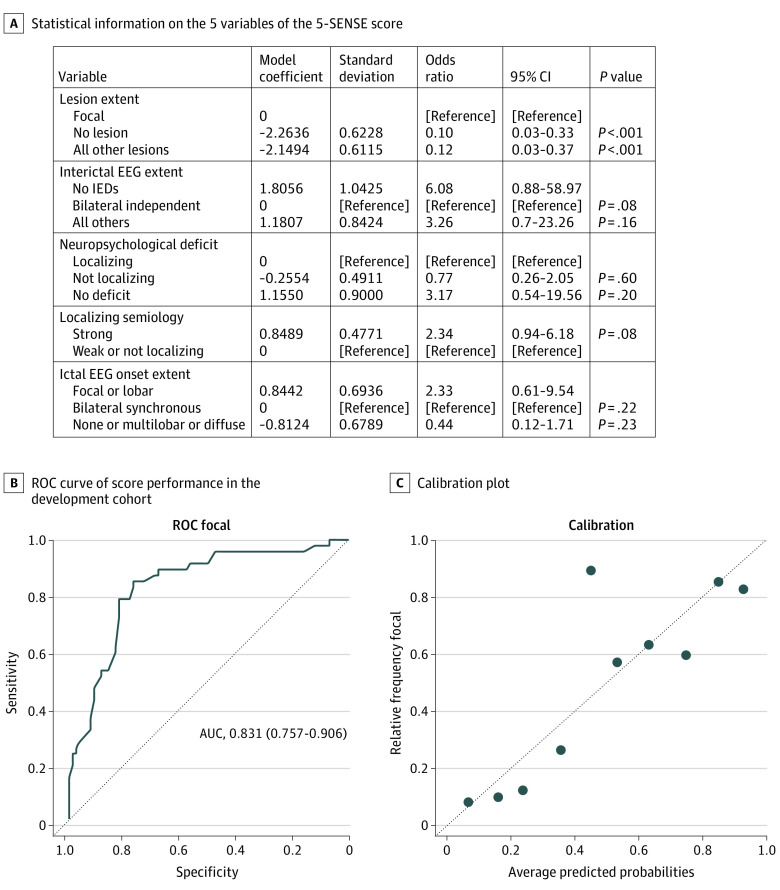
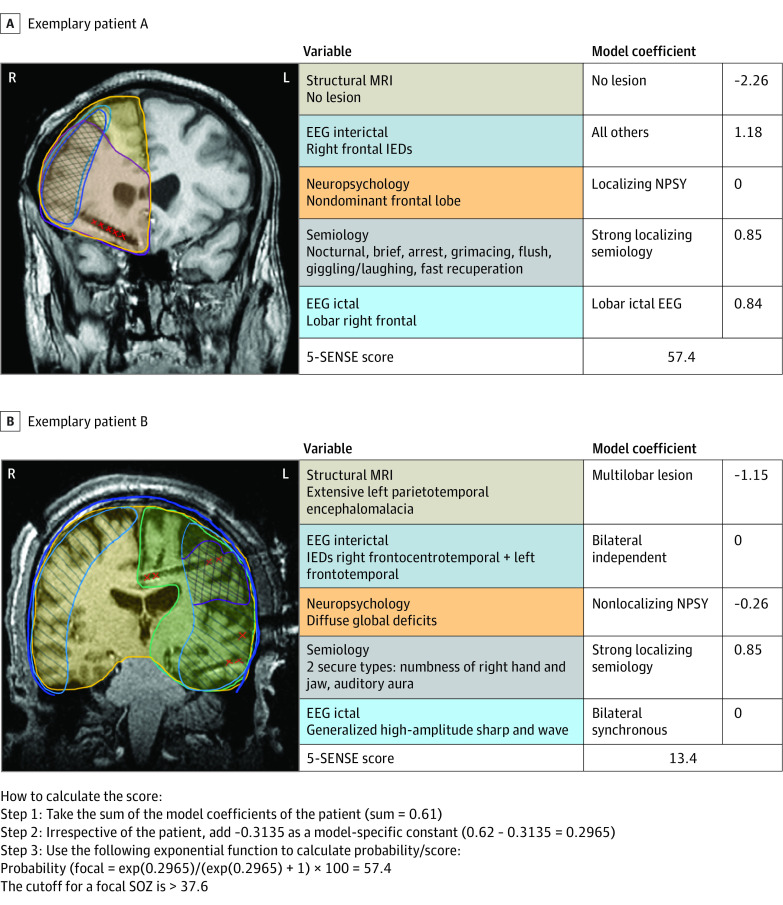
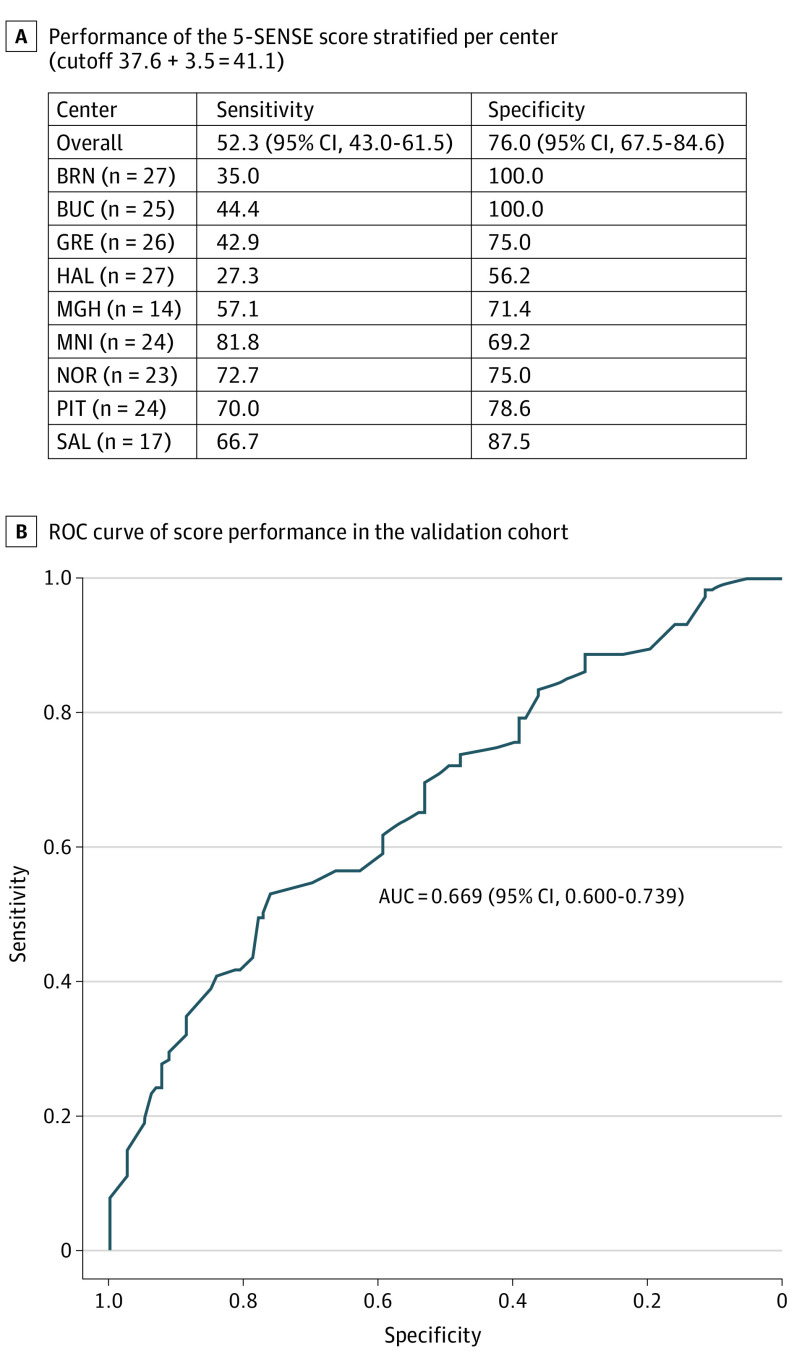
Results: A total of 128 patients (57 women [44.5%]; median [range] age, 31 [13-58] years) were analyzed for score development and 207 patients (97 women [46.9%]; median [range] age, 32 [16-70] years) were analyzed for validation. The score comprised the following 5 predictive variables: focal lesion on structural magnetic resonance imaging, absence of bilateral independent spikes in scalp electroencephalography, localizing neuropsychological deficit, strongly localizing semiology, and regional ictal scalp electroencephalography onset. The 5-SENSE score had an optimal mean (SD) probability cutoff for identifying a focal seizure-onset zone of 37.6 (3.5). Area under the curve, specificity, and sensitivity were 0.83, 76.3% (95% CI, 66.7-85.8), and 83.3% (95% CI, 72.30-94.1), respectively. Validation showed 76.0% (95% CI, 67.5-84.0) specificity and 52.3% (95% CI, 43.0-61.5) sensitivity.
Conclusions and relevance: High specificity in score development and validation confirms that the 5-SENSE score predicts patients where SEEG is unlikely to identify a focal seizure-onset zone. It is a simple and useful tool for assisting clinicians to reduce unnecessary invasive diagnostic burden on patients and overutilization of limited health care resources.
Conflict of interest statement
Figures
Comment in
-
Nomograms Should Not Be Used by General Neurologists When Considering Referral for Epilepsy Surgery.Epilepsy Curr. 2022 Dec 22;23(2):93-94. doi: 10.1177/15357597221145263. eCollection 2023 Mar-Apr. Epilepsy Curr. 2022. PMID: 37122411 Free PMC article. No abstract available.
References
-
- Lüders HO, Najm I, Nair D, Widdess-Walsh P, Bingman W. The epileptogenic zone: general principles. Epileptic Disord. 2006;8(suppl 2):S1-S9. - PubMed
