

Comparison of Ticagrelor vs Clopidogrel in Addition to Aspirin in Patients With Minor Ischemic Stroke and Transient Ischemic Attack: A Network Meta-analysis
- PMID: 34870698
- PMCID: PMC8649906
- DOI: 10.1001/jamaneurol.2021.4514
Comparison of Ticagrelor vs Clopidogrel in Addition to Aspirin in Patients With Minor Ischemic Stroke and Transient Ischemic Attack: A Network Meta-analysis
Abstract
Importance: Dual antiplatelet therapy (DAPT) with clopidogrel and aspirin is effective in preventing recurrent strokes after minor ischemic stroke or transient ischemic attack (TIA). However, there is emerging evidence for the use of ticagrelor and aspirin, and the 2 DAPT regimens have not been compared directly.
Objective: To compare ticagrelor and aspirin with clopidogrel and aspirin in patients with acute minor ischemic stroke or TIA in the prevention of recurrent strokes or death.
Data sources: MEDLINE, Embase, and Cochrane from database inception until February 2021.
Study selection: Randomized clinical trials that enrolled adults with acute minor ischemic stroke or TIA and provided the mentioned interventions within 72 hours of symptom onset, with a minimum follow-up of 30 days.
Data extraction and synthesis: PRISMA guidelines for network meta-analyses were followed. Two reviewers independently extracted data and appraised risk of bias. Fixed-effects models were fit using a bayesian approach to network meta-analysis. Between-group comparisons were estimated using hazard ratios (HRs) with 95% credible intervals (95% CrIs). Surface under the cumulative rank curve plots were produced.
Main outcomes and measures: The primary outcome was a composite of recurrent stroke or death up to 90 days. Secondary outcomes include major bleeding, mortality, adverse events, and functional disability. A sensitivity analysis was performed at 30 days for the primary outcome.
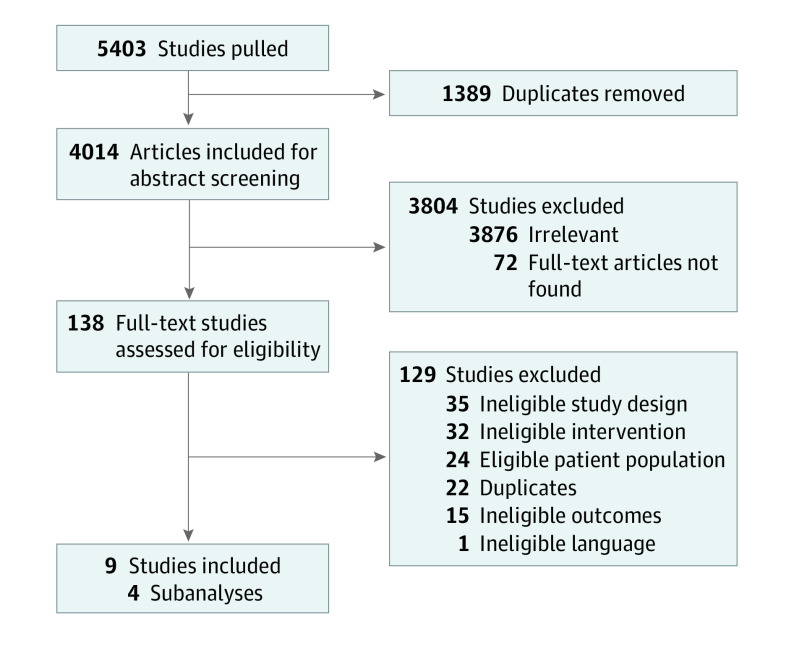
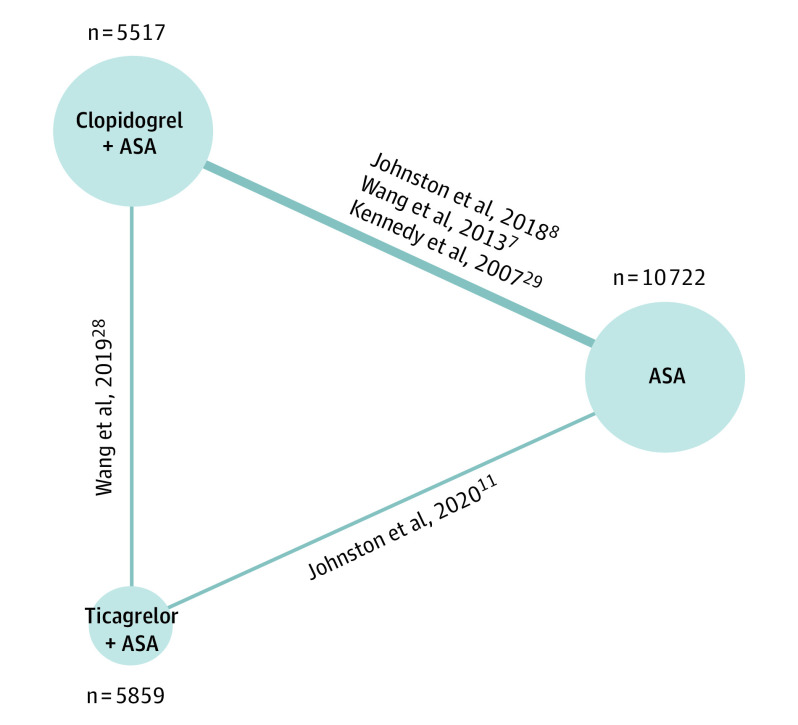
Results: A total of 4014 citations were screened; 5 randomized clinical trials were included. Data from 22 098 patients were analyzed, including 5517 in the clopidogrel and aspirin arm, 5859 in the ticagrelor and aspirin arm, and 10 722 in the aspirin arm. Both clopidogrel and aspirin (HR, 0.74; 95% CrI, 0.65-0.84) and ticagrelor and aspirin (HR, 0.79; 95% CrI, 0.68-0.91) were superior to aspirin in the prevention of recurrent stroke and death. There was no statistically significant difference between clopidogrel and aspirin compared with ticagrelor and aspirin (HR, 0.94; 95% CrI, 0.78-1.13). Both DAPT regimens had higher rates of major hemorrhage than aspirin alone. Clopidogrel and aspirin was associated with a decreased risk of functional disability compared with aspirin alone (HR, 0.82; 95% CrI, 0.74-0.91) and ticagrelor and aspirin (HR, 0.85; 95% CrI, 0.75-0.97).
Conclusions and relevance: DAPT combining aspirin with either ticagrelor or clopidogrel was superior to aspirin alone, but there was no statistically significant difference found between the 2 regimens for the primary outcome.
Conflict of interest statement
Figures
References
-
- Amarenco P, Lavallée PC, Monteiro Tavares L, et al. ; TIAregistry.org Investigators . Five-year risk of stroke after TIA or minor ischemic stroke. N Engl J Med. 2018;378(23):2182-2190. doi: 10.1056/NEJMoa1802712 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
