

Superior vena cava graft infection in thoracic surgery: a retrospective study of the French EPITHOR database
- PMID: 34871387
- PMCID: PMC8860414
- DOI: 10.1093/icvts/ivab337
Superior vena cava graft infection in thoracic surgery: a retrospective study of the French EPITHOR database
Abstract
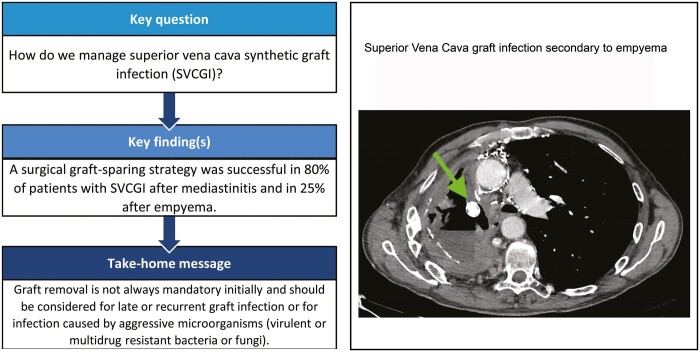
Objectives: To report our experience on the management of superior vena cava graft infection.
Methods: Between 2001 and 2018, patients with superior vena cava synthetic graft or patch reconstruction after resection of intrathoracic tumours or benign disease were selected retrospectively from the French EPITHOR database and participating thoracic centres. Our study population includes patients with superior vena cava graft infection, defined according to the MAGIC consensus. Superior vena cava synthetic grafts in an empyema or mediastinitis were considered as infected.
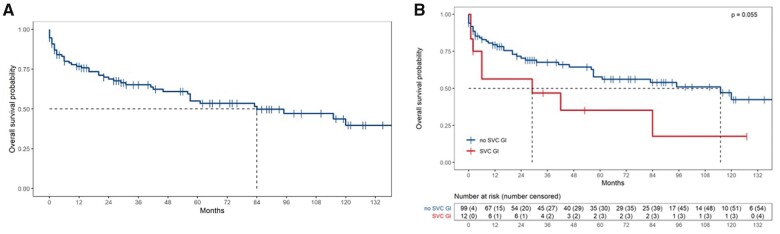
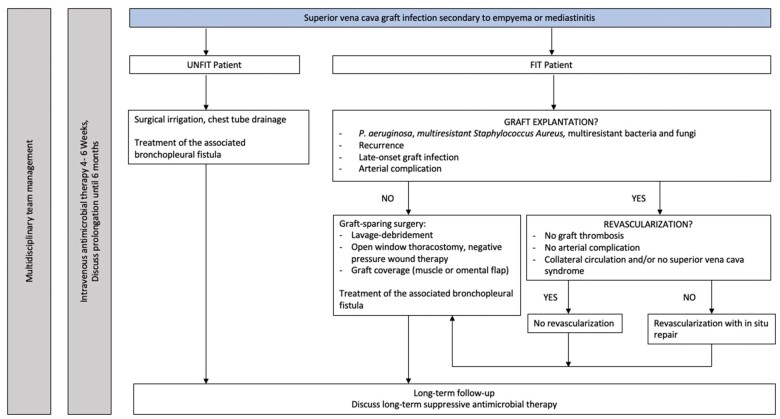
Results: Of 111 eligible patients, superior vena cava graft infection occurred in 12 (11.9%) patients with a polytetrafluoroethylene graft secondary to contiguous contamination. Management consisted of either conservative treatment with chest tube drainage and antibiotics (n = 3) or a surgical graft-sparing strategy (n = 9). Recurrence of infection appears in 6 patients. Graft removal was performed in 2 patients among the 5 reoperated patients. The operative mortality rate was 25%.
Conclusions: Superior vena cava graft infection may develop as a surgical site infection secondary to early mediastinitis or empyema. Graft removal is not always mandatory but should be considered in late or recurrent graft infection or in infections caused by aggressive microorganisms (virulent or multidrug resistant bacteria or fungi).
Keywords: Empyema; Graft infection; Mediastinal tumours; Mediastinitis; Non-small-cell lung cancer; Superior vena cava reconstruction.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures

Similar articles
-
Surgical reconstruction of the superior vena cava.Cardiovasc Surg. 1994 Oct;2(5):598-604. Cardiovasc Surg. 1994. PMID: 7820520
-
Bypass of superior vena cava. Fifteen years' experience with spiral vein graft for obstruction of superior vena cava caused by benign disease.J Thorac Cardiovasc Surg. 1990 May;99(5):889-95; discussion 895-6. J Thorac Cardiovasc Surg. 1990. PMID: 2329828
-
Upper thoracic empyema and concomitant superior vena cava syndrome treated with reconstructive surgery using a pedicled omental flap.Nagoya J Med Sci. 2022 Aug;84(3):648-655. doi: 10.18999/nagjms.84.3.648. Nagoya J Med Sci. 2022. PMID: 36237890 Free PMC article.
-
[Surgical vein reconstruction in patients with tumor invasiveness of the superior caval system. Retrospective study of 7 cases].J Chir (Paris). 1996 Apr;133(2):61-4. J Chir (Paris). 1996. PMID: 8763562 Review. French.
-
Tuberculosis lymphadenopathy: A rare etiology of the superior vena cava syndrome.J Med Vasc. 2021 Feb;46(1):9-12. doi: 10.1016/j.jdmv.2020.11.001. Epub 2020 Dec 2. J Med Vasc. 2021. PMID: 33546823 Review.
References
-
- Dartevelle PG, Mitilian D, Fadel E.. Extended surgery for T4 lung cancer: a 30 years’ experience. Gen Thorac Cardiovasc Surg 2017;65:321–8. - PubMed
-
- Sekine Y, Suzuki H, Saitoh Y, Wada H, Yoshida S.. Prosthetic reconstruction of the superior vena cava for malignant disease: surgical techniques and outcomes. Ann Thorac Surg 2010;90:223–8. - PubMed
-
- Spaggiari L, Magdeleinat P, Kondo H, Thomas P, Leon ME, Rollet G. et al. Results of superior vena cava resection for lung cancer. Analysis of prognostic factors. Lung Cancer 2004;44:339–46. - PubMed
-
- Dartevelle PG, Chapelier AR, Pastorino U, Corbi P, Lenot B, Cerrina J. et al. Long-term follow-up after prosthetic replacement of the superior vena cava combined with resection of mediastinal-pulmonary malignant tumors. J Thorac Cardiovasc Surg 1991;102:259–65. - PubMed
-
- Bernard A, Rivera C, Pages PB, Falcoz PE, Vicaut E, Dahan M.. Risk model of in-hospital mortality after pulmonary resection for cancer: a national database of the French Society of Thoracic and Cardiovascular Surgery (Epithor). J Thorac Cardiovasc Surg 2011;141:449–58. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
