

Kidney Recovery and Death in Critically Ill Patients With COVID-19-Associated Acute Kidney Injury Treated With Dialysis: The STOP-COVID Cohort Study
- PMID: 34871701
- PMCID: PMC8641974
- DOI: 10.1053/j.ajkd.2021.11.004
Kidney Recovery and Death in Critically Ill Patients With COVID-19-Associated Acute Kidney Injury Treated With Dialysis: The STOP-COVID Cohort Study
Abstract
Rationale & objective: Acute kidney injury treated with kidney replacement therapy (AKI-KRT) occurs frequently in critically ill patients with coronavirus disease 2019 (COVID-19). We examined the clinical factors that determine kidney recovery in this population.
Study design: Multicenter cohort study.
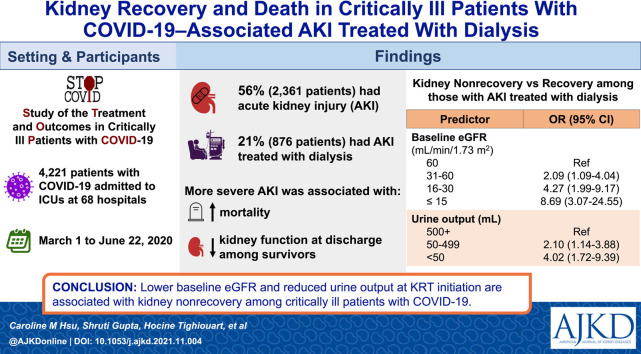
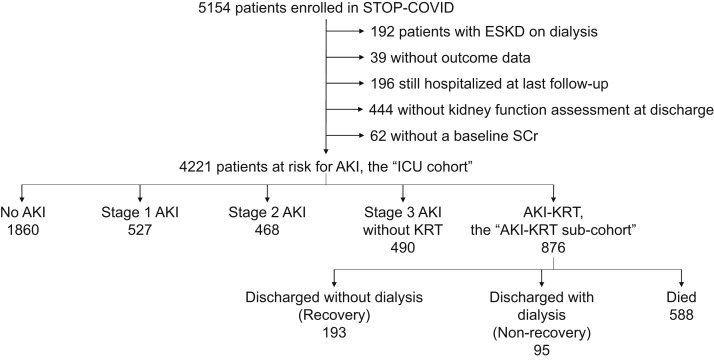
Setting & participants: 4,221 adults not receiving KRT who were admitted to intensive care units at 68 US hospitals with COVID-19 from March 1 to June 22, 2020 (the "ICU cohort"). Among these, 876 developed AKI-KRT after admission to the ICU (the "AKI-KRT subcohort").
Exposure: The ICU cohort was analyzed using AKI severity as the exposure. For the AKI-KRT subcohort, exposures included demographics, comorbidities, initial mode of KRT, and markers of illness severity at the time of KRT initiation.
Outcome: The outcome for the ICU cohort was estimated glomerular filtration rate (eGFR) at hospital discharge. A 3-level outcome (death, kidney nonrecovery, and kidney recovery at discharge) was analyzed for the AKI-KRT subcohort.
Analytical approach: The ICU cohort was characterized using descriptive analyses. The AKI-KRT subcohort was characterized with both descriptive analyses and multinomial logistic regression to assess factors associated with kidney nonrecovery while accounting for death.
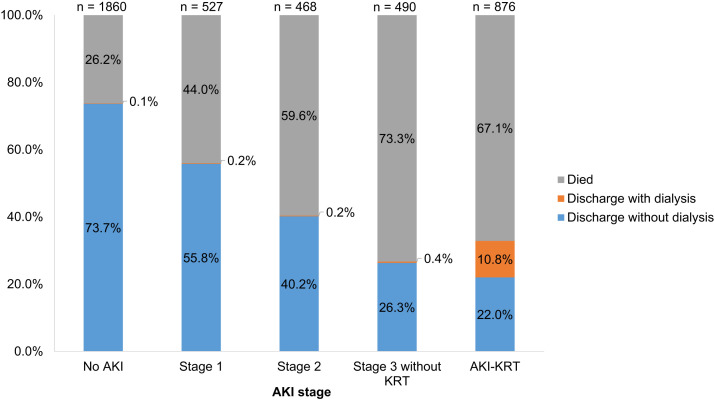
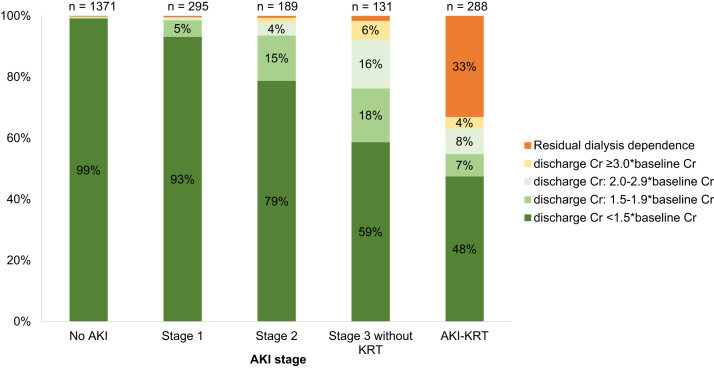
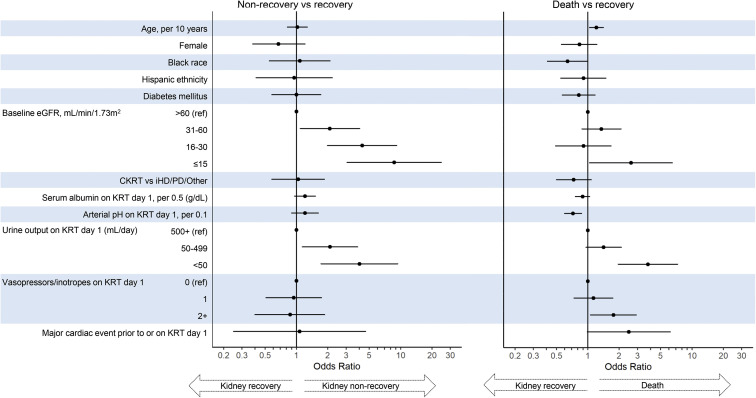
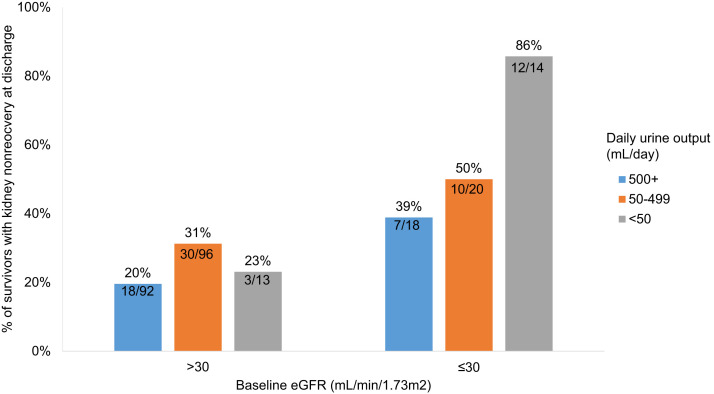
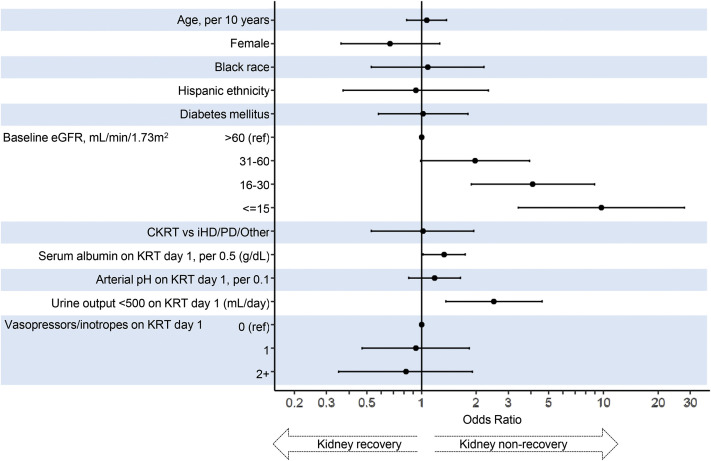
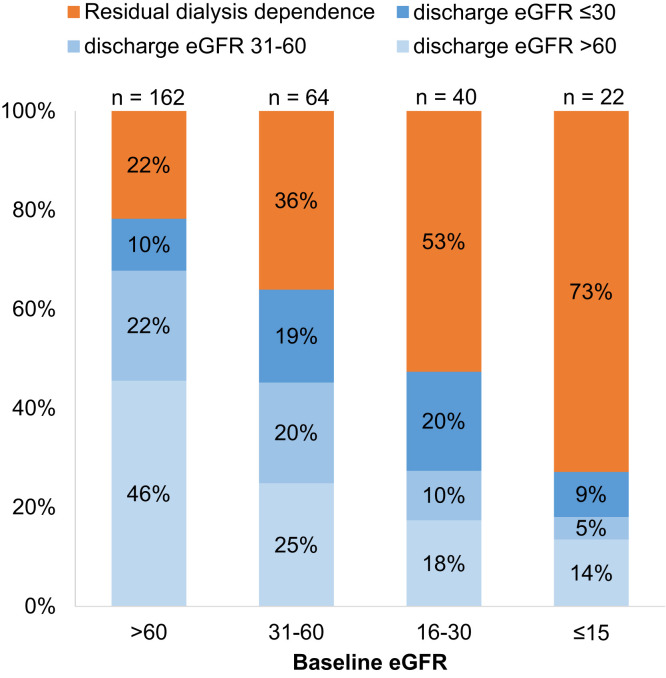
Results: Among a total of 4,221 patients in the ICU cohort, 2,361 (56%) developed AKI, including 876 (21%) who received KRT. More severe AKI was associated with higher mortality. Among survivors, more severe AKI was associated with an increased rate of kidney nonrecovery and lower kidney function at discharge. Among the 876 patients with AKI-KRT, 588 (67%) died, 95 (11%) had kidney nonrecovery, and 193 (22%) had kidney recovery by the time of discharge. The odds of kidney nonrecovery was greater for lower baseline eGFR, with ORs of 2.09 (95% CI, 1.09-4.04), 4.27 (95% CI, 1.99-9.17), and 8.69 (95% CI, 3.07-24.55) for baseline eGFR 31-60, 16-30, ≤15 mL/min/1.73 m2, respectively, compared with eGFR > 60 mL/min/1.73 m2. Oliguria at the time of KRT initiation was also associated with nonrecovery (ORs of 2.10 [95% CI, 1.14-3.88] and 4.02 [95% CI, 1.72-9.39] for patients with 50-499 and <50 mL/d of urine, respectively, compared to ≥500 mL/d of urine).
Limitations: Later recovery events may not have been captured due to lack of postdischarge follow-up.
Conclusions: Lower baseline eGFR and reduced urine output at the time of KRT initiation are each strongly and independently associated with kidney nonrecovery among critically ill patients with COVID-19.
Keywords: Acute kidney injury (AKI); chronic kidney disease (CKD); coronavirus disease 2019 (COVID-19); critical care; dialysis; estimated glomerular filtration rate (eGFR); oligoanuria; prognostication; renal function; renal recovery; urine output.
Copyright © 2021 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
