

Preconception care and severe maternal morbidity in the United States
- PMID: 34871778
- PMCID: PMC8891086
- DOI: 10.1016/j.ajogmf.2021.100549
Preconception care and severe maternal morbidity in the United States
Abstract
Background: In the United States, approximately 52,000 women per year (accounting for 1.46% of births) experience severe maternal morbidity, which is defined as a complication that causes significant maternal harm or risk of death. It disproportionately affects women from racial or ethnic minorities, people with chronic diseases, and those with Medicaid or no insurance. Preconception care has been hailed as a strategy to improve pregnancy outcomes and reduce disparities, but its broad benefits for maternal outcomes have not been demonstrated.
Objective: Our objective was to measure the association between preconception care and the odds of severe maternal morbidity among women with Medicaid.
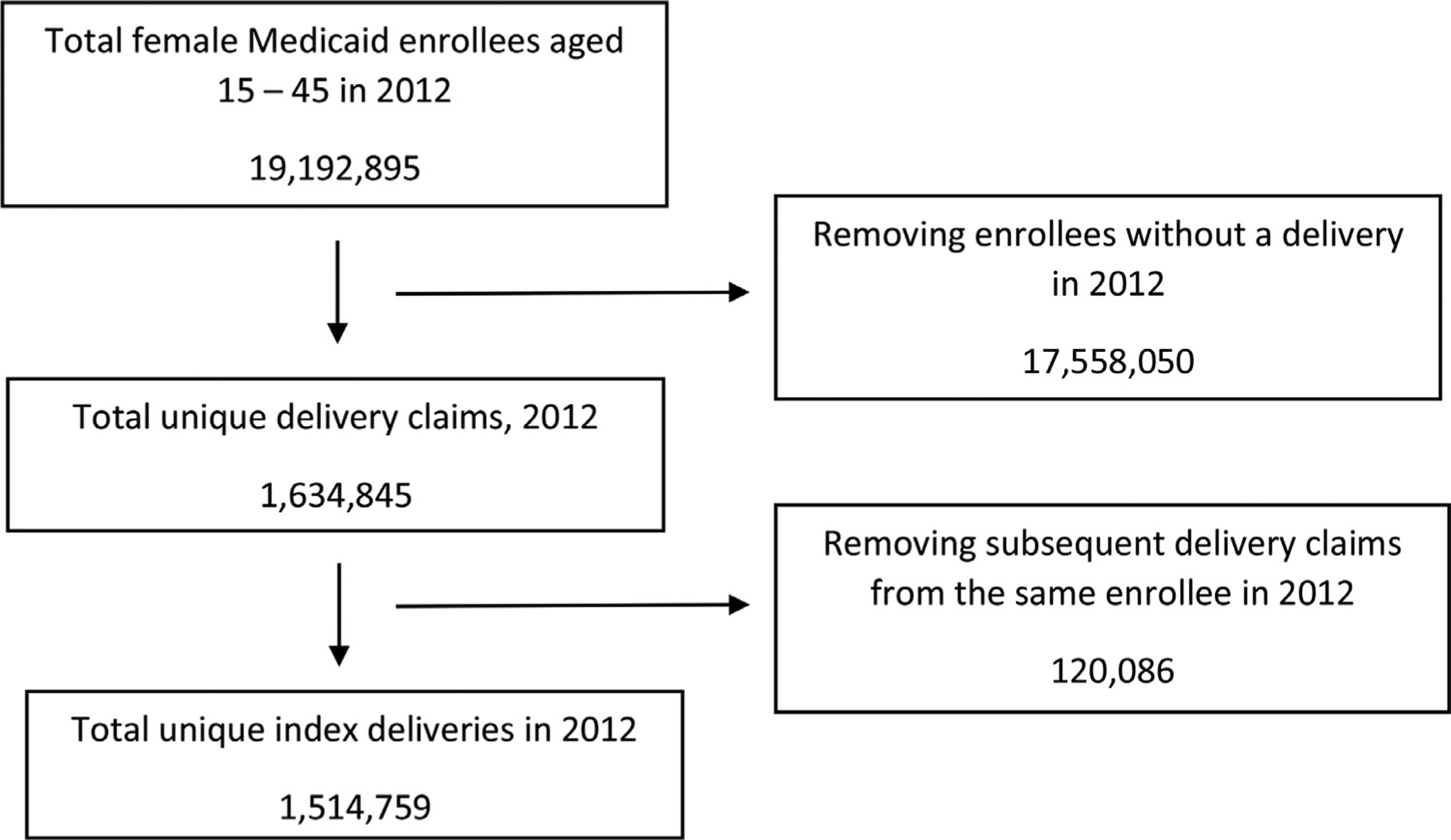
Study design: This is a secondary analysis of Medicaid claims using the Medicaid Analytic Extract files (2010-2012). We used the International Classification of Diseases, Ninth Revision codes, published by the US Office of Population Affairs' Quality Family Planning program to define 7 domains of preconception care. The primary outcome was maternal death within 12 weeks of delivery or severe maternal morbidity during birth hospitalization, defined by the presence of any diagnosis or procedure on the severe maternal morbidity International Classification of Diseases, Ninth Revision code list from the Centers for Disease Control and Prevention. Because this list may overestimate severe maternal morbidity by counting any blood transfusion, our secondary outcome used the same code list but without transfusion. We reviewed care in the year before conception and used logistic regression to estimate the association between each domain and severe maternal morbidity for all births to women enrolled in Medicaid and aged 15 to 45 years with births during 2012. We performed a subgroup analysis for women with chronic disease (kidney disease, hypertension, or diabetes).
Results: Severe maternal morbidity or death occurred in 26,285 births (1.74%) when including blood transfusions and 9,481 births (0.63%) when excluding transfusions. Receiving contraceptive services in the year before conception was associated with decreased odds of severe maternal morbidity (adjusted odds ratio, 0.92; 95% confidence interval, 0.88-0.95) and pregnancy test services were associated with increased odds (adjusted odds ratio, 1.08; 95% confidence interval, 1.01-1.14). In the primary analysis, no significant associations were observed for other preconception care domains. Among those women with at least 1 chronic disease, contraceptive care (adjusted odds ratio, 0.84; 95% confidence interval, 0.75-0.95) and routine physical or gynecologic exams (adjusted odds ratio, 0.79; 95% confidence interval, 0.71-0.88) were associated with decreased odds of severe maternal morbidity. Similar associations were found for severe maternal morbidity when excluding blood transfusion.
Conclusions: Contraceptive services in the year before conception and routine exams for women with chronic disease are associated with decreased odds of severe maternal morbidity or death for Medicaid enrollees.
Keywords: Medicaid; contraception; maternal morbidity; preconception care.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors report no conflict of interest.
Figures
Similar articles
-
Increased risk of severe maternal morbidity among infertile women: analysis of US claims data.Am J Obstet Gynecol. 2020 Sep;223(3):404.e1-404.e20. doi: 10.1016/j.ajog.2020.02.027. Epub 2020 Feb 27. Am J Obstet Gynecol. 2020. PMID: 32112734 Free PMC article.
-
Association of preconception paternal health and adverse maternal outcomes among healthy mothers.Am J Obstet Gynecol MFM. 2021 Sep;3(5):100384. doi: 10.1016/j.ajogmf.2021.100384. Epub 2021 Apr 23. Am J Obstet Gynecol MFM. 2021. PMID: 33895399
-
Assessment of Incidence and Factors Associated With Severe Maternal Morbidity After Delivery Discharge Among Women in the US.JAMA Netw Open. 2021 Feb 1;4(2):e2036148. doi: 10.1001/jamanetworkopen.2020.36148. JAMA Netw Open. 2021. PMID: 33528553 Free PMC article.
-
Preconception indicators and associations with health outcomes reported in UK routine primary care data: a systematic review.Br J Gen Pract. 2025 Jan 30;75(751):e129-e136. doi: 10.3399/BJGP.2024.0082. Print 2025 Feb. Br J Gen Pract. 2025. PMID: 38950944 Free PMC article.
-
Innovations in Preconception Care: Optimizing Health for All Individuals.J Midwifery Womens Health. 2024 Nov-Dec;69(6):897-905. doi: 10.1111/jmwh.13681. Epub 2024 Aug 6. J Midwifery Womens Health. 2024. PMID: 39104297 Free PMC article. Review.
Cited by
-
A blueprint for a new model of sexual and reproductive health care in subspecialty medicine.Health Serv Res. 2023 Feb;58(1):216-222. doi: 10.1111/1475-6773.14074. Epub 2022 Oct 11. Health Serv Res. 2023. PMID: 36151999 Free PMC article. No abstract available.
-
Severe Maternal Morbidity in Georgia, 2009-2020.Med Care. 2023 May 1;61(5):258-267. doi: 10.1097/MLR.0000000000001819. Epub 2023 Jan 11. Med Care. 2023. PMID: 36638324 Free PMC article.
-
Care of pregnant women with pre-existing medical conditions in German perinatal centers.Arch Gynecol Obstet. 2025 Jul;312(1):267-272. doi: 10.1007/s00404-025-08016-4. Epub 2025 Apr 7. Arch Gynecol Obstet. 2025. PMID: 40195199 Free PMC article.
-
Screening to understand pregnancy preferences and offer referrals and treatment (SUPPORT): Results of a pilot quality improvement initiative.PLoS One. 2024 Jul 29;19(7):e0303930. doi: 10.1371/journal.pone.0303930. eCollection 2024. PLoS One. 2024. PMID: 39074124 Free PMC article.
-
Racial and Socioeconomic Disparities in Preconception Health Risk Factors and Access to Care.J Womens Health (Larchmt). 2024 Aug;33(8):1063-1071. doi: 10.1089/jwh.2023.0560. Epub 2024 Apr 1. J Womens Health (Larchmt). 2024. PMID: 38563909 Free PMC article.
References
-
- Callaghan WM, Creanga AA, Kuklina EV. Severe maternal morbidity among delivery and postpartum hospitalizations in the United States. Obstet Gynecol 2012;120:1029–36. - PubMed
-
- Fingar KR, Hambrick MM, Heslin KC, Moore JE. Trends and disparities in delivery hospitalizations involving severe maternal morbidity, 2006–2015: statistical brief #243. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018. September 4. - PubMed
-
- World Health Organization. Trends in maternal mortality: 1990–2015: estimates from WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. World Health Organization; 2015.
-
- Creanga AA, Bateman BT, Kuklina EV, Callaghan WM. Racial and ethnic disparities in severe maternal morbidity: a multistate analysis, 2008–2010. Am J Obstet Gynecol 2014;210: 435.. e1–8. - PubMed
-
- Creanga AA, Berg CJ, Syverson C, Seed K, Bruce FC, Race Callaghan WM. ethnicity, and nativity differentials in pregnancy-related mortality in the United States: 1993–2006. Obstet Gynecol 2012;120:261–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
