

Capillary hemodynamics and contracting skeletal muscle oxygen pressures in male rats with heart failure: Impact of soluble guanylyl cyclase activator
- PMID: 34871799
- PMCID: PMC9469501
- DOI: 10.1016/j.niox.2021.12.001
Capillary hemodynamics and contracting skeletal muscle oxygen pressures in male rats with heart failure: Impact of soluble guanylyl cyclase activator
Abstract
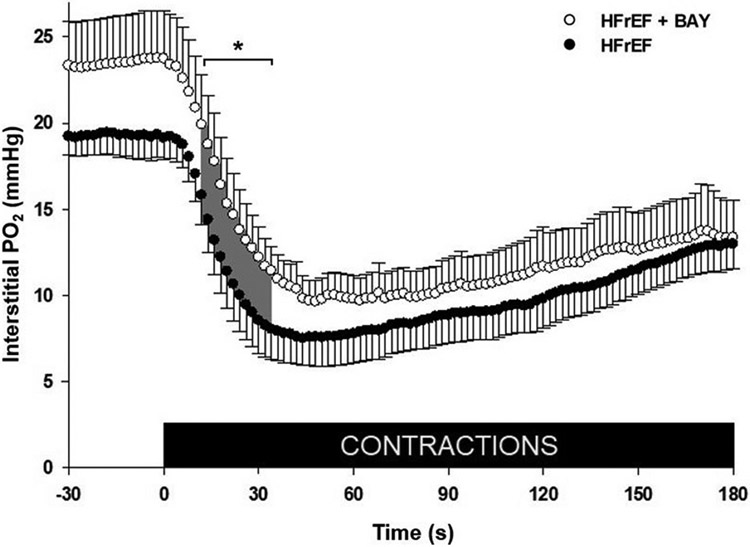
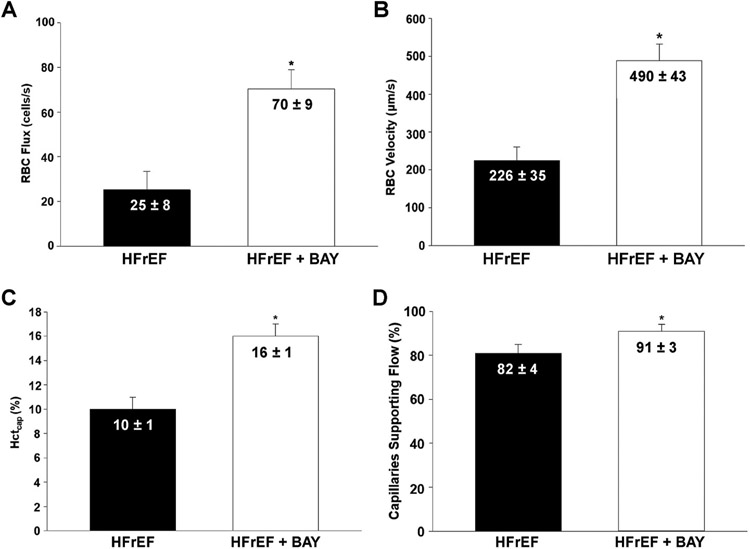
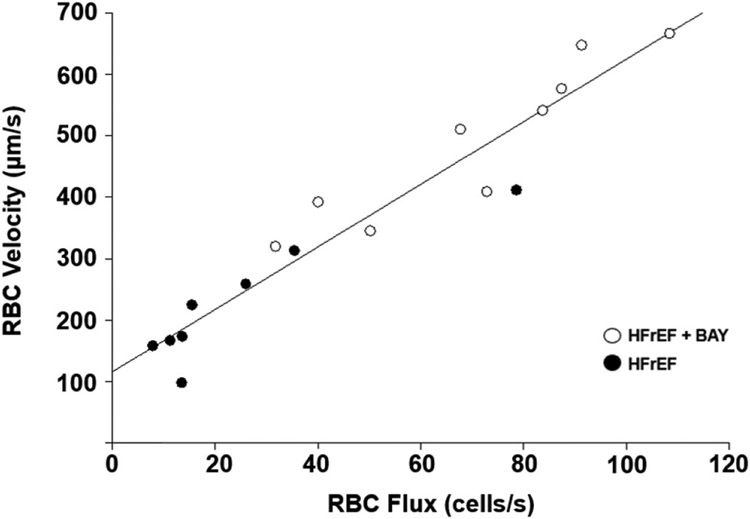
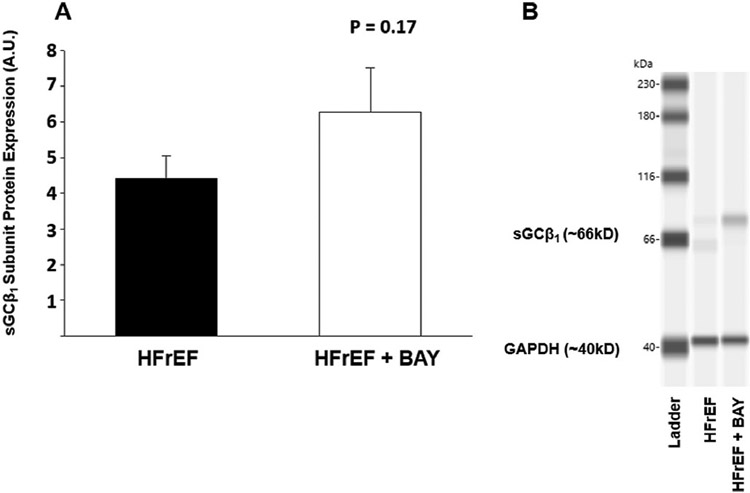
In heart failure with reduced ejection fraction (HFrEF), nitric oxide-soluble guanylyl cyclase (sGC) pathway dysfunction impairs skeletal muscle arteriolar vasodilation and thus capillary hemodynamics, contributing to impaired oxygen uptake (V̇O2) kinetics. Targeting this pathway with sGC activators offers a new treatment approach to HFrEF. We tested the hypotheses that sGC activator administration would increase the O2 delivery (Q̇O2)-to-V̇O2 ratio in the skeletal muscle interstitial space (PO2is) of HFrEF rats during twitch contractions due, in part, to increases in red blood cell (RBC) flux (fRBC), velocity (VRBC), and capillary hematocrit (Hctcap). HFrEF was induced in male Sprague-Dawley rats via myocardial infarction. After 3 weeks, rats were treated with 0.3 mg/kg of the sGC activator BAY 60-2770 (HFrEF + BAY; n = 11) or solvent (HFrEF; n = 9) via gavage b.i.d for 5 days prior to phosphorescence quenching (PO2is, in contracting muscle) and intravital microscopy (resting) measurements in the spinotrapezius muscle. Intravital microscopy revealed higher fRBC (70 ± 9 vs 25 ± 8 RBC/s), VRBC (490 ± 43 vs 226 ± 35 μm/s), Hctcap (16 ± 1 vs 10 ± 1%) and a greater number of capillaries supporting flow (91 ± 3 vs 82 ± 3%) in HFrEF + BAY vs HFrEF (all P < 0.05). Additionally, PO2is was especially higher during 12-34s of contractions in HFrEF + BAY vs HFrEF (P < 0.05). Our findings suggest that sGC activators improved resting Q̇O2 via increased fRBC, VRBC, and Hctcap allowing for better Q̇O2-to-V̇O2 matching during the rest-contraction transient, supporting sGC activators as a potential therapeutic to target skeletal muscle vasomotor dysfunction in HFrEF.
Keywords: Exercise; Microcirculation; Nitric oxide; Oxygen transport.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Regulation of capillary hemodynamics by KATP channels in resting skeletal muscle.Physiol Rep. 2021 Apr;9(8):e14803. doi: 10.14814/phy2.14803. Physiol Rep. 2021. PMID: 33932103 Free PMC article.
-
Effects of pulmonary hypertension on microcirculatory hemodynamics in rat skeletal muscle.Microvasc Res. 2022 May;141:104334. doi: 10.1016/j.mvr.2022.104334. Epub 2022 Jan 30. Microvasc Res. 2022. PMID: 35104507 Free PMC article.
-
Sexual dimorphism in the control of skeletal muscle interstitial Po2 of heart failure rats: effects of dietary nitrate supplementation.J Appl Physiol (1985). 2019 May 1;126(5):1184-1192. doi: 10.1152/japplphysiol.01004.2018. Epub 2019 Mar 7. J Appl Physiol (1985). 2019. PMID: 30844332 Free PMC article.
-
A Multicenter, Randomized, Double-Blind, Placebo-Controlled Trial of the Efficacy and Safety of the Oral Soluble Guanylate Cyclase Stimulator: The VICTORIA Trial.JACC Heart Fail. 2018 Feb;6(2):96-104. doi: 10.1016/j.jchf.2017.08.013. Epub 2017 Oct 11. JACC Heart Fail. 2018. PMID: 29032136 Review.
-
Novel sGC Stimulators and sGC Activators for the Treatment of Heart Failure.Handb Exp Pharmacol. 2017;243:225-247. doi: 10.1007/164_2016_100. Handb Exp Pharmacol. 2017. PMID: 27900610 Review.
Cited by
-
Capillary-Mitochondrial Oxygen Transport in Muscle: Paradigm Shifts.Function (Oxf). 2023 Mar 16;4(3):zqad013. doi: 10.1093/function/zqad013. eCollection 2023. Function (Oxf). 2023. PMID: 37168497 Free PMC article. Review.
-
Oxygen transport across the lifespan of male Sprague Dawley rats.Biogerontology. 2025 Jan 8;26(1):38. doi: 10.1007/s10522-024-10180-0. Biogerontology. 2025. PMID: 39775306
References
-
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain A, Chang A, Chang S, Das S, Delling F, Djousse L, Ferguson J, Fornage M, Jordan L, Khan S, Kissela B, Knutson K, Kwan T, Lackland D, Lewis T, Lichtman J, Longenecker C, Loop M, Lutsey P, Martin S, Matsushita K, Moran A, Mussolino M, O’Flaherty M, Pandry A, Perak A, Rosamond W, Roth G, Sampson U, Satou G, Schroeder E, Shah S, Spartano N, Stokes A, Tirschwell D, Tsao C, Turakhia M, VanWagner L, Wilkins J, Wong S, Virani S, American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee, Heart disease and stroke statistics—2019 update: a report from the American Heart Association, Circulation 139 (10) (2019) e56–e528, 2019. - PubMed
-
- Weber KT, Kinasewitz GT, Janicki JS, Fishman AP, Oxygen utilization and ventilation during exercise in patients with chronic cardiac failure, Circulation 65 (6) (1982) 1213–1223. - PubMed
-
- Crespo-Leiro MG, Metra M, Lund LH, Milicic D, Costanzo MR, Filippatos G, Gustafsson F, Tsui S, Barge-Caballero E, De Jonge N, Frigerio M, Hamdan R, Hasin T, Hülsmann M, Nalbantgil S, Potena L, Bauersachs J, Gkouziouta A, Ruhparwar A, Ristic AD, Straburzynska-Migaj E, Mcdonagh T, Serferovic P, Ruschitzka F, Advanced heart failure: a position statement of the heart failure association of the European society of cardiology, Eur. J. Heart Fail 20 (11) (2018) 1505–1535. - PubMed
-
- Drexler H, Hayoz D, Münzel T, Hornig B, Just H, Brunner HR, Zelis R, Endothelial function in chronic congestive heart failure, Am. J. Cardiol 69 (19) (1992) 1596–1601. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
