

Severity of respiratory failure and computed chest tomography in acute COVID-19 correlates with pulmonary function and respiratory symptoms after infection with SARS-CoV-2: An observational longitudinal study over 12 months
- PMID: 34871947
- PMCID: PMC8632363
- DOI: 10.1016/j.rmed.2021.106709
Severity of respiratory failure and computed chest tomography in acute COVID-19 correlates with pulmonary function and respiratory symptoms after infection with SARS-CoV-2: An observational longitudinal study over 12 months
Abstract
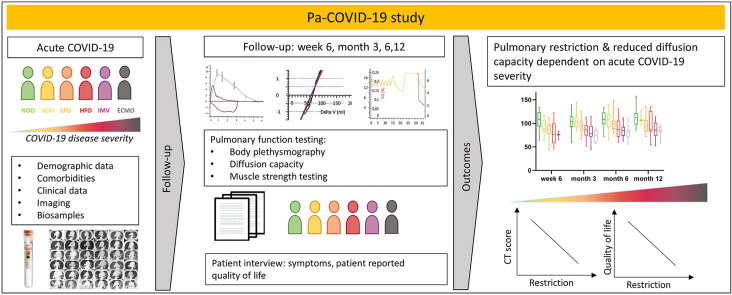
Introduction: Prospective and longitudinal data on pulmonary injury over one year after acute coronavirus disease 2019 (COVID-19) are sparse. We aim to determine reductions in pulmonary function and respiratory related quality of life up to 12 months after acute COVID-19.
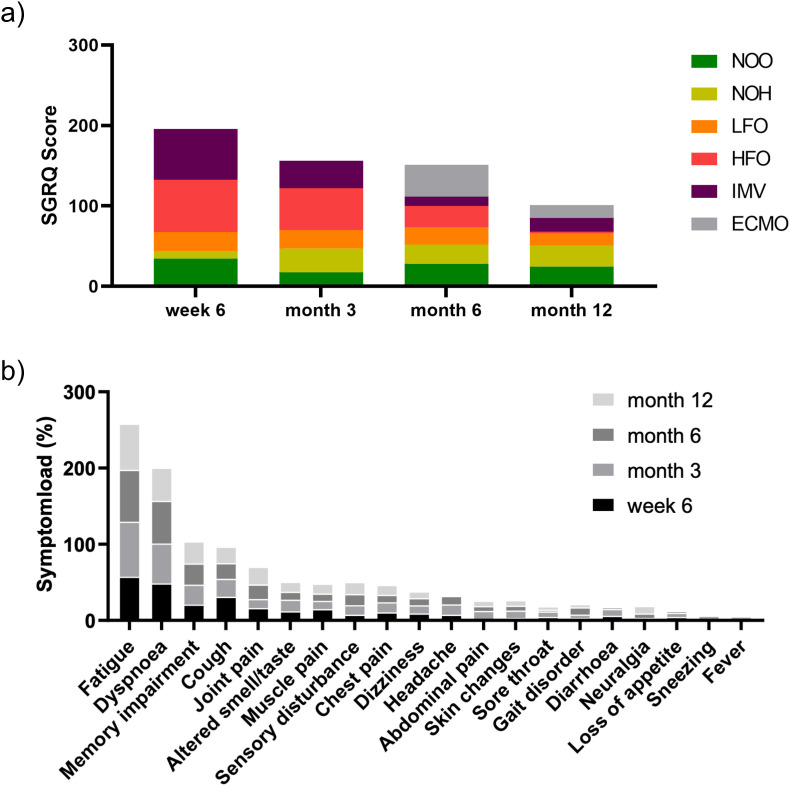
Methods: Patients with acute COVID-19 were enrolled into an ongoing single-centre, prospective observational study and prospectively examined 6 weeks, 3, 6 and 12 months after onset of COVID-19 symptoms. Chest CT-scans, pulmonary function and symptoms assessed by St. Georges Respiratory Questionnaire were used to evaluate respiratory limitations. Patients were stratified according to severity of acute COVID-19.
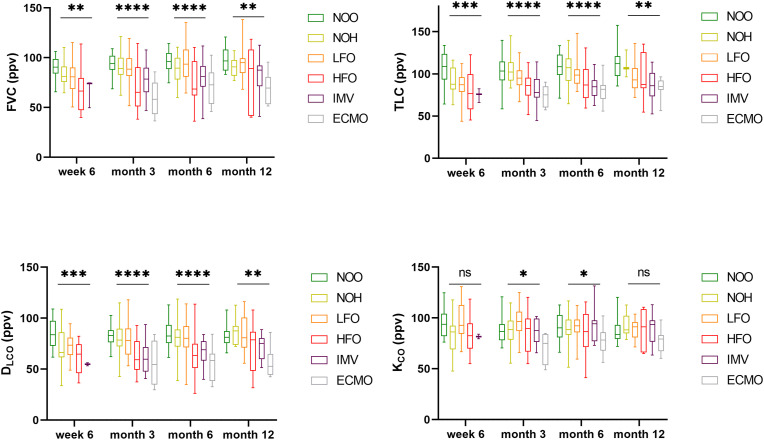
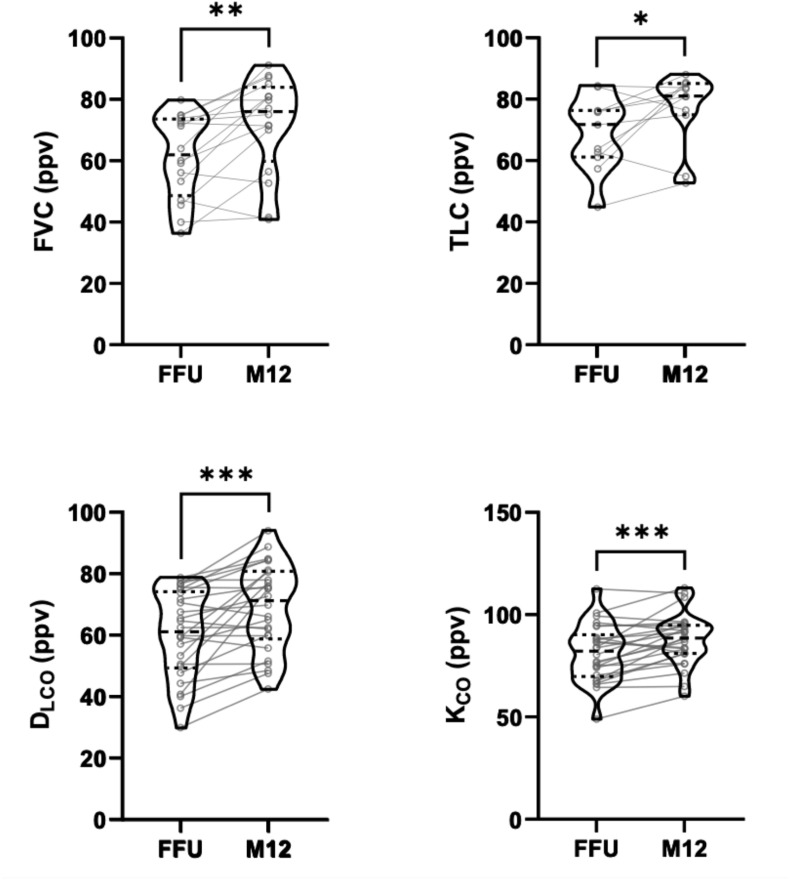
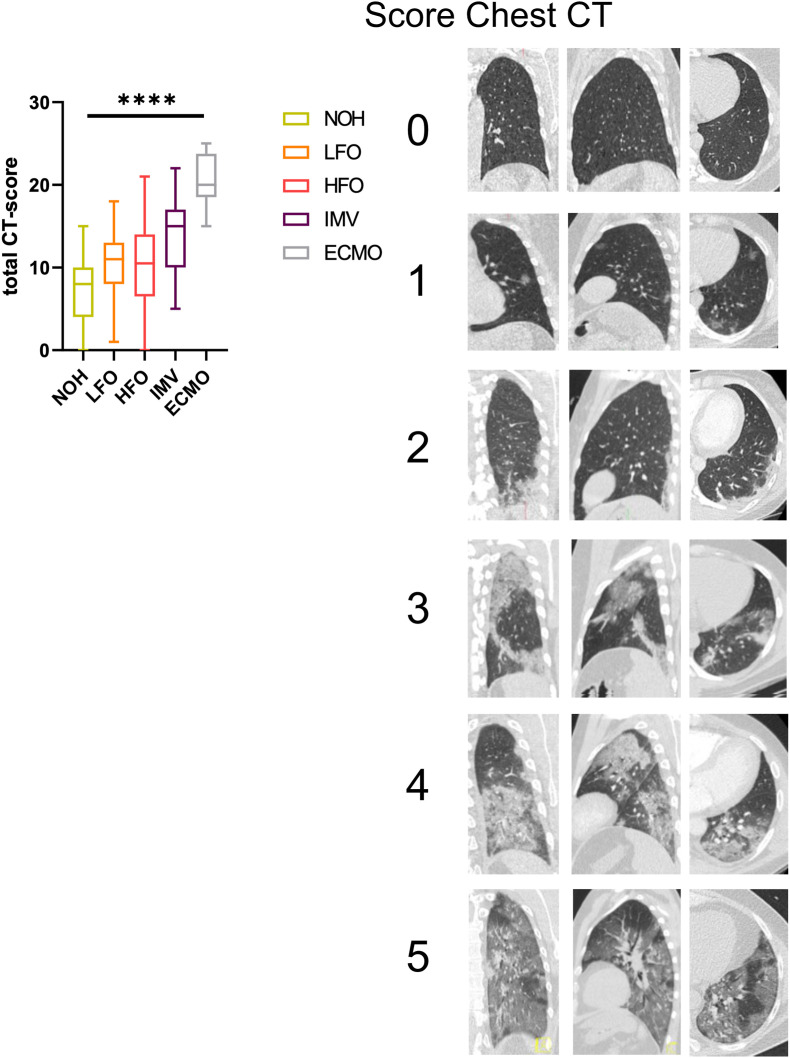
Results: Median age of all patients was 57 years, 37.8% were female. Higher age, male sex and higher BMI were associated with acute-COVID-19 severity (p < 0.0001, 0.001 and 0.004 respectively). Also, pulmonary restriction and reduced carbon monoxide diffusion capacity was associated with disease severity. In patients with restriction and impaired diffusion capacity, FVC improved over 12 months from 61.32 to 71.82, TLC from 68.92 to 76.95, DLCO from 60.18 to 68.98 and KCO from 81.28 to 87.80 (percent predicted values; p = 0.002, 0.045, 0.0002 and 0.0005). The CT-score of lung involvement in the acute phase was associated with restriction and reduction in diffusion capacity in follow-up. Respiratory symptoms improved for patients in higher severity groups during follow-up, but not for patients with initially mild disease.
Conclusion: Severity of respiratory failure during COVID-19 correlates with the degree of pulmonary function impairment and respiratory quality of life in the year after acute infection.
Keywords: COVID-19; Long-COVID; Pneumonia; Post-COVID; Post-acute COVID; Pulmonary function; Pulmonary outcome; Pulmonary restriction; Pulmonary sequelae; Quality of life; SARS-CoV-2.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
M.W. received funding for research from Deutsche Forschungsgemeinschaft, Bundesministerium für Bildung und Forschung, Deutsche Gesellschaft für Pneumologie, European Respiratory Society, Marie Curie Foundation, Else Kröner Fresenius Stiftung, Capnetz Stiftung, International Max Planck Research School, Actelion, Bayer Health Care, Biotest, Boehringer Ingelheim, Noxxon, Pantherna, Quark Pharma, Silence Therapeutics, Takeda Pharma, Vaxxilon, and for lectures and advisory from Actelion, Alexion, Aptarion, Astra Zeneca, Bayer Health Care, Berlin Chemie, Biotest, Boehringer Ingelheim, Chiesi, Glaxo Smith Kline, Insmed, Novartis, Teva and Vaxxilon. T.Z. received funding for research from Bundesministerium für Bildung und Forschung, Else Kröner-Fresenius Stiftung and Gesellschaft für Internationale Zusammenarbeit.
Figures

Similar articles
-
Long-Term Pulmonary Sequelae and Immunological Markers in Patients Recovering from Severe and Critical COVID-19 Pneumonia: A Comprehensive Follow-Up Study.Medicina (Kaunas). 2024 Nov 27;60(12):1954. doi: 10.3390/medicina60121954. Medicina (Kaunas). 2024. PMID: 39768836 Free PMC article.
-
Correlation of the severity of the clinical presentation of SARS-CoV-2 pneumonia with respiratory function parameters in the post-COVID period.J Infect Dev Ctries. 2024 Sep 30;18(9):1347-1352. doi: 10.3855/jidc.19471. J Infect Dev Ctries. 2024. PMID: 39436850
-
A Follow-Up Study of Lung Function and Chest Computed Tomography at 6 Months after Discharge in Patients with Coronavirus Disease 2019.Can Respir J. 2021 Feb 13;2021:6692409. doi: 10.1155/2021/6692409. eCollection 2021. Can Respir J. 2021. PMID: 33628349 Free PMC article.
-
Respiratory function in patients post-infection by COVID-19: a systematic review and meta-analysis.Pulmonology. 2021 Jul-Aug;27(4):328-337. doi: 10.1016/j.pulmoe.2020.10.013. Epub 2020 Nov 25. Pulmonology. 2021. PMID: 33262076 Free PMC article.
-
Pulmonary function and chest computed tomography abnormalities 6-12 months after recovery from COVID-19: a systematic review and meta-analysis.Respir Res. 2022 Sep 6;23(1):233. doi: 10.1186/s12931-022-02163-x. Respir Res. 2022. PMID: 36068582 Free PMC article.
Cited by
-
Metabolic disorders and post-acute hospitalization in black/mixed-race patients with long COVID in Brazil: A cross-sectional analysis.PLoS One. 2022 Oct 31;17(10):e0276771. doi: 10.1371/journal.pone.0276771. eCollection 2022. PLoS One. 2022. PMID: 36315558 Free PMC article.
-
Assessment of Pulmonary Function Tests in COVID-19 Convalescents Six Months after Infection.J Clin Med. 2022 Nov 29;11(23):7052. doi: 10.3390/jcm11237052. J Clin Med. 2022. PMID: 36498626 Free PMC article.
-
Autophagy in Inflammatory Response against SARS-CoV-2.Int J Mol Sci. 2023 Mar 3;24(5):4928. doi: 10.3390/ijms24054928. Int J Mol Sci. 2023. PMID: 36902354 Free PMC article. Review.
-
Lung function and quality of life one year after severe COVID-19 in Brazil.J Bras Pneumol. 2024 May 27;50(2):e20230261. doi: 10.36416/1806-3756/e20230261. eCollection 2024. J Bras Pneumol. 2024. PMID: 38808823 Free PMC article.
-
Fatigue outcomes following COVID-19: a systematic review and meta-analysis.BMJ Open. 2023 Apr 26;13(4):e063969. doi: 10.1136/bmjopen-2022-063969. BMJ Open. 2023. PMID: 37185637 Free PMC article.
References
-
- Wiersinga W.J., Rhodes A., Cheng A.C., et al. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. J. Am. Med. Assoc. 2020;324(8):782–793. - PubMed
-
- Wölfel R., Corman V.M., Guggemos W., et al. Virological assessment of hospitalized patients with COVID-2019. Nature. 2020;581(7809):465–469. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
