

Methods for Monitoring Risk of Hypoxic Damage in Fetal and Neonatal Brains: A Review
- PMID: 34872080
- PMCID: PMC8983560
- DOI: 10.1159/000520987
Methods for Monitoring Risk of Hypoxic Damage in Fetal and Neonatal Brains: A Review
Abstract
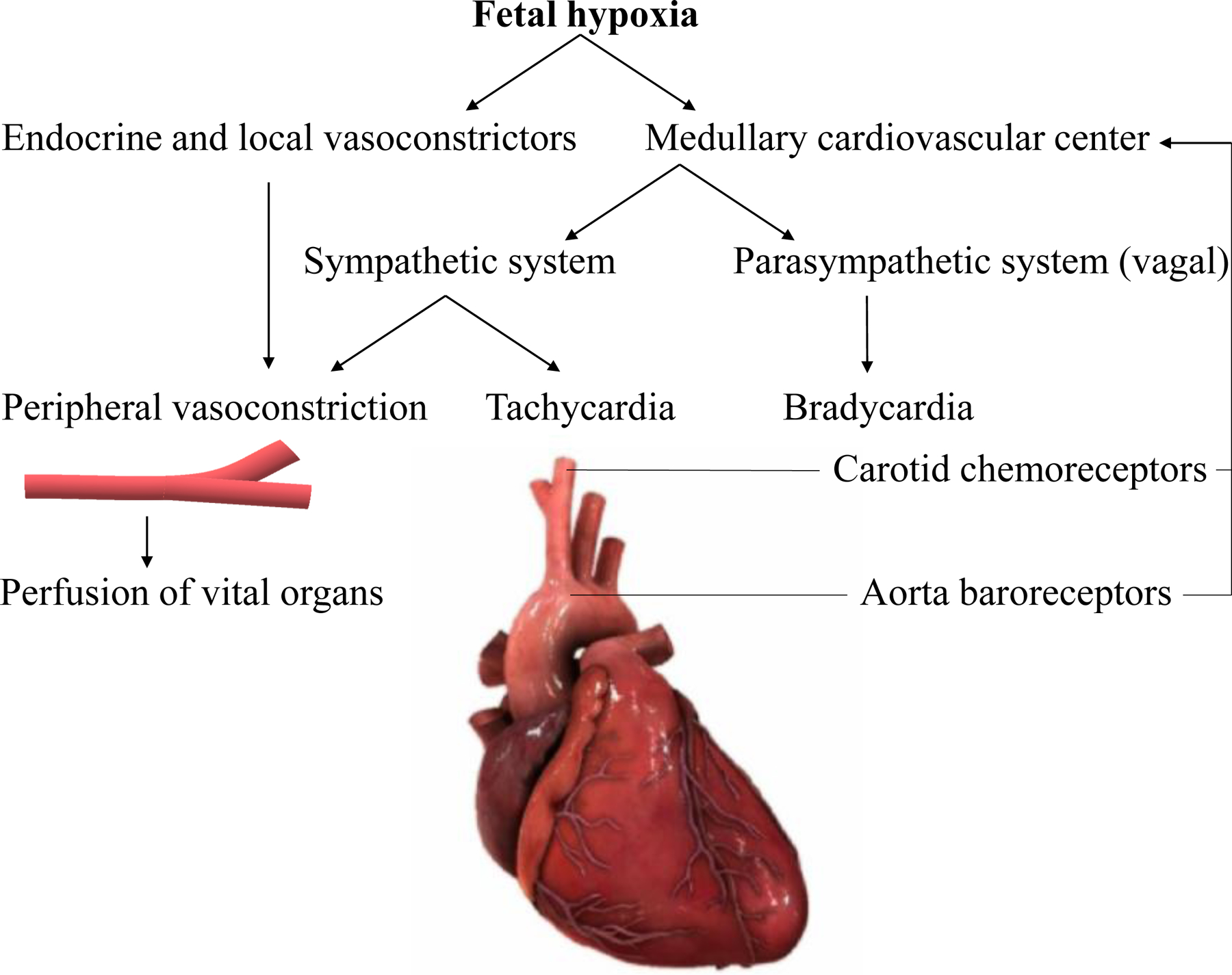
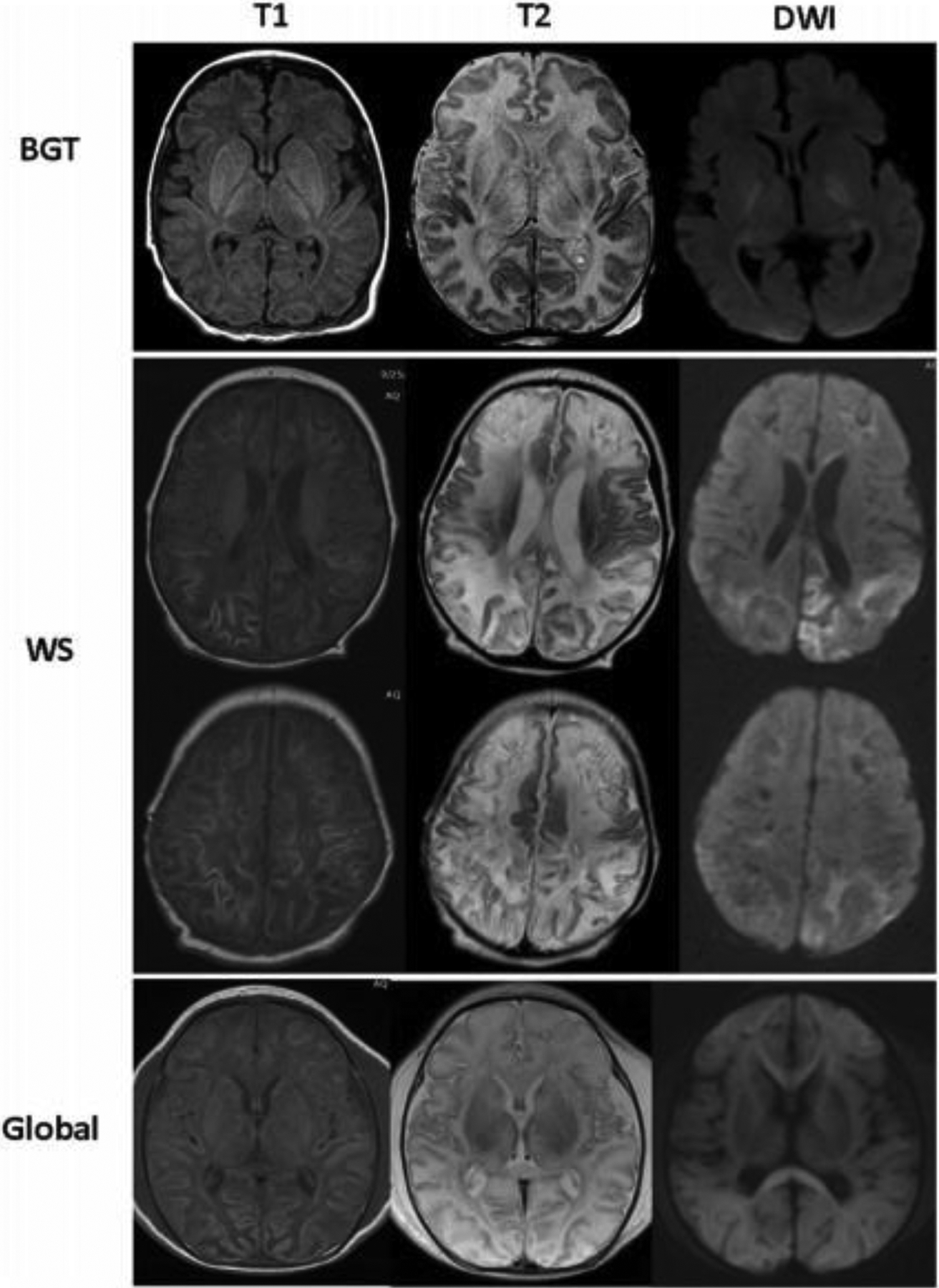
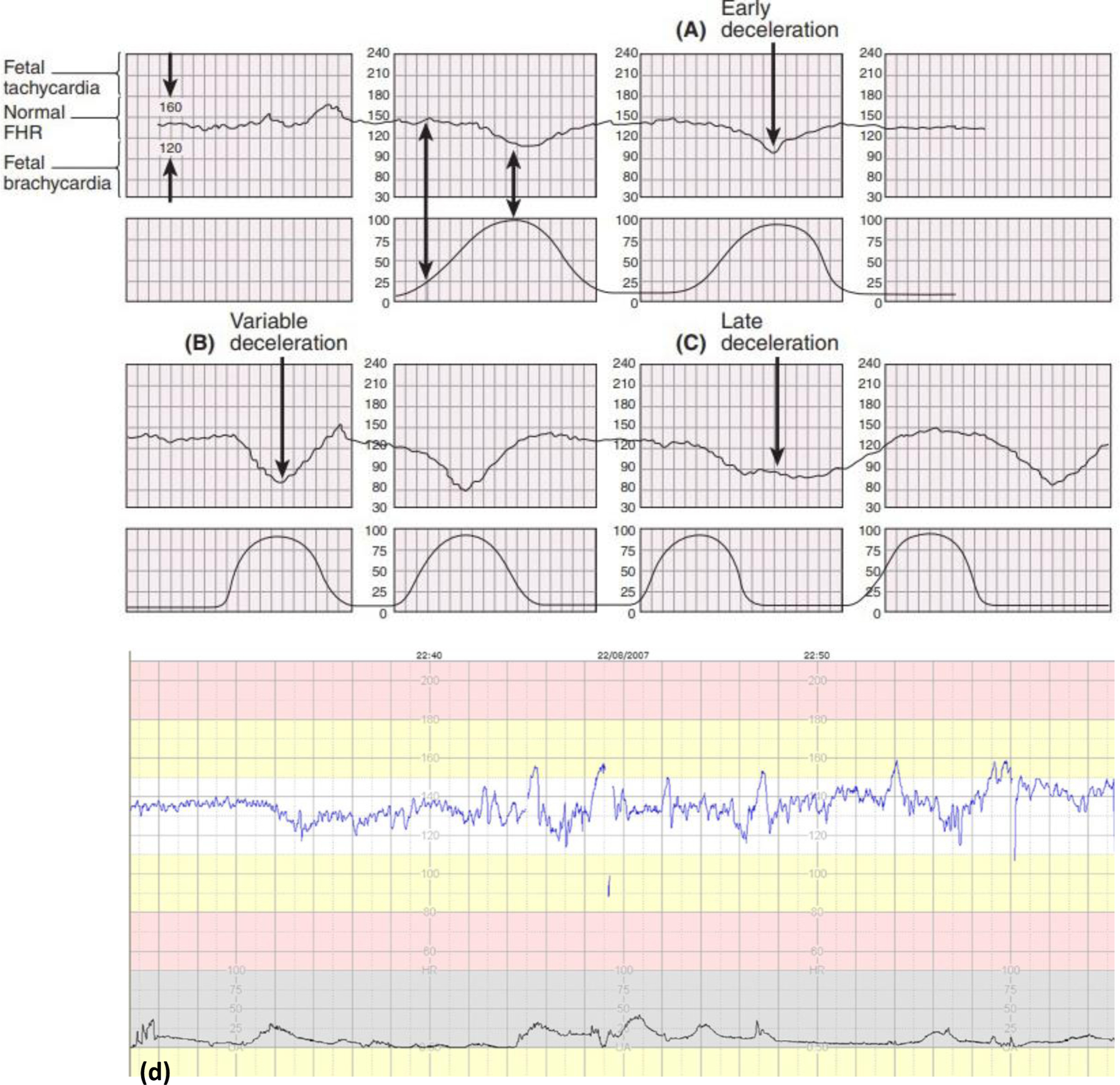
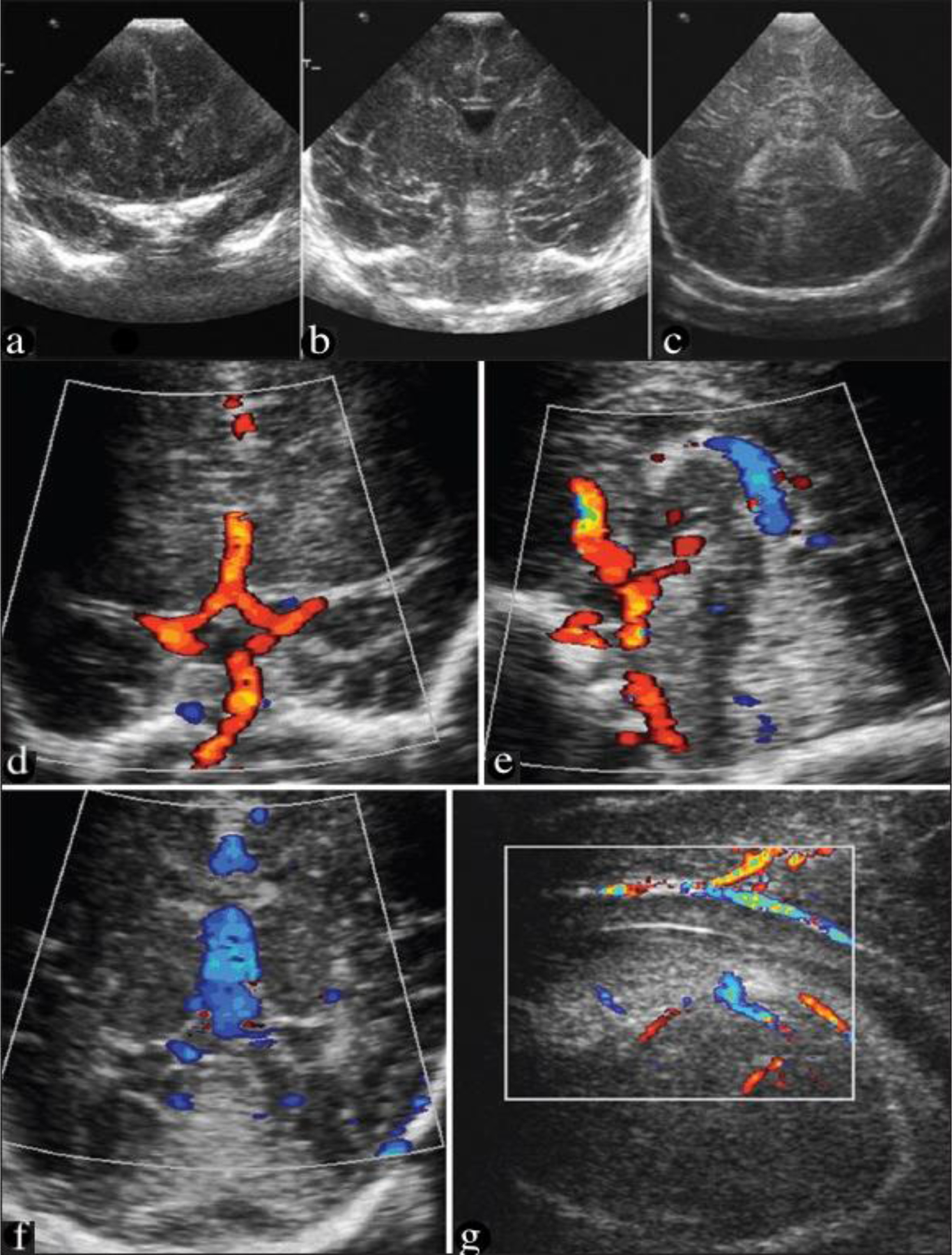
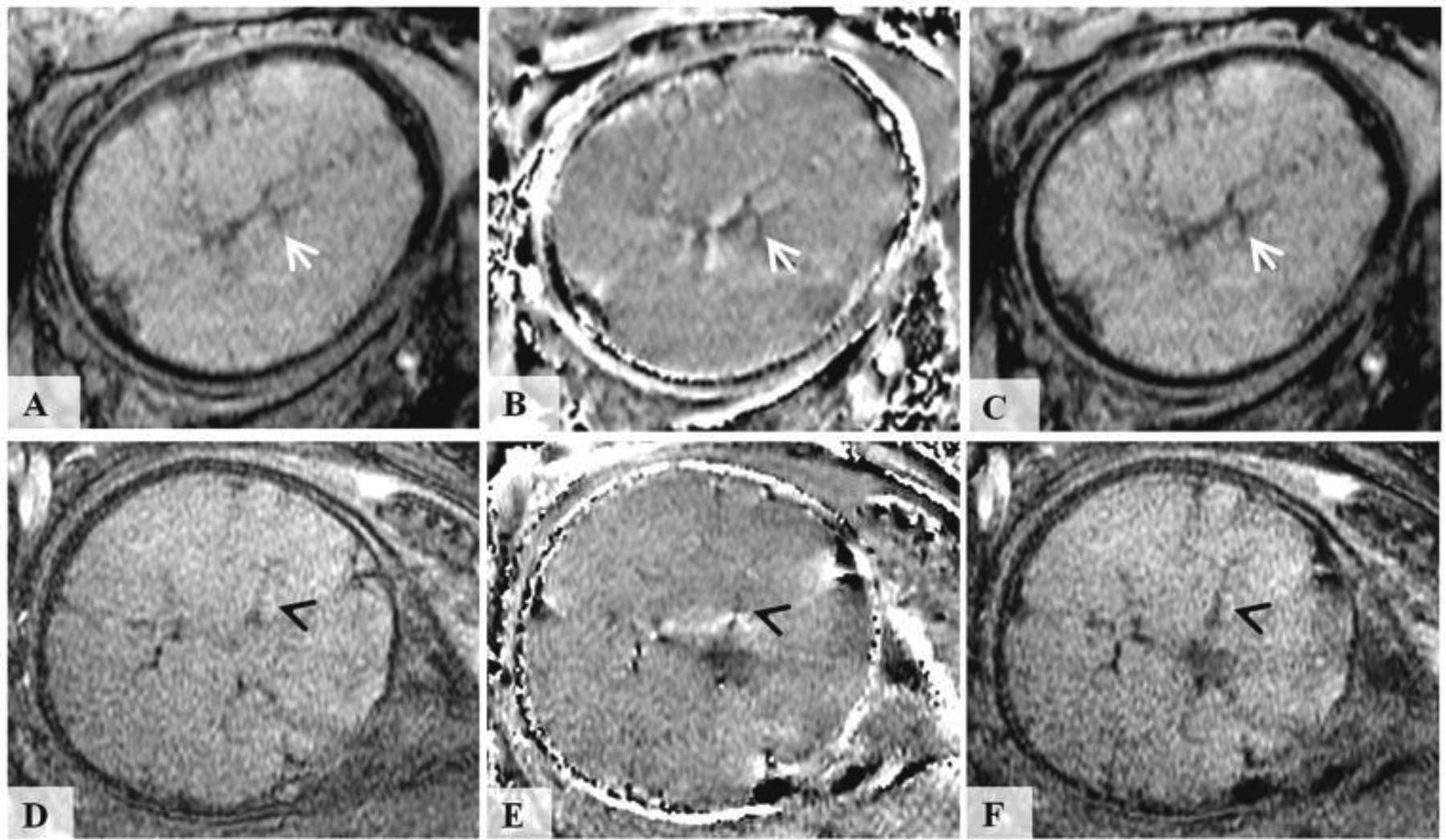
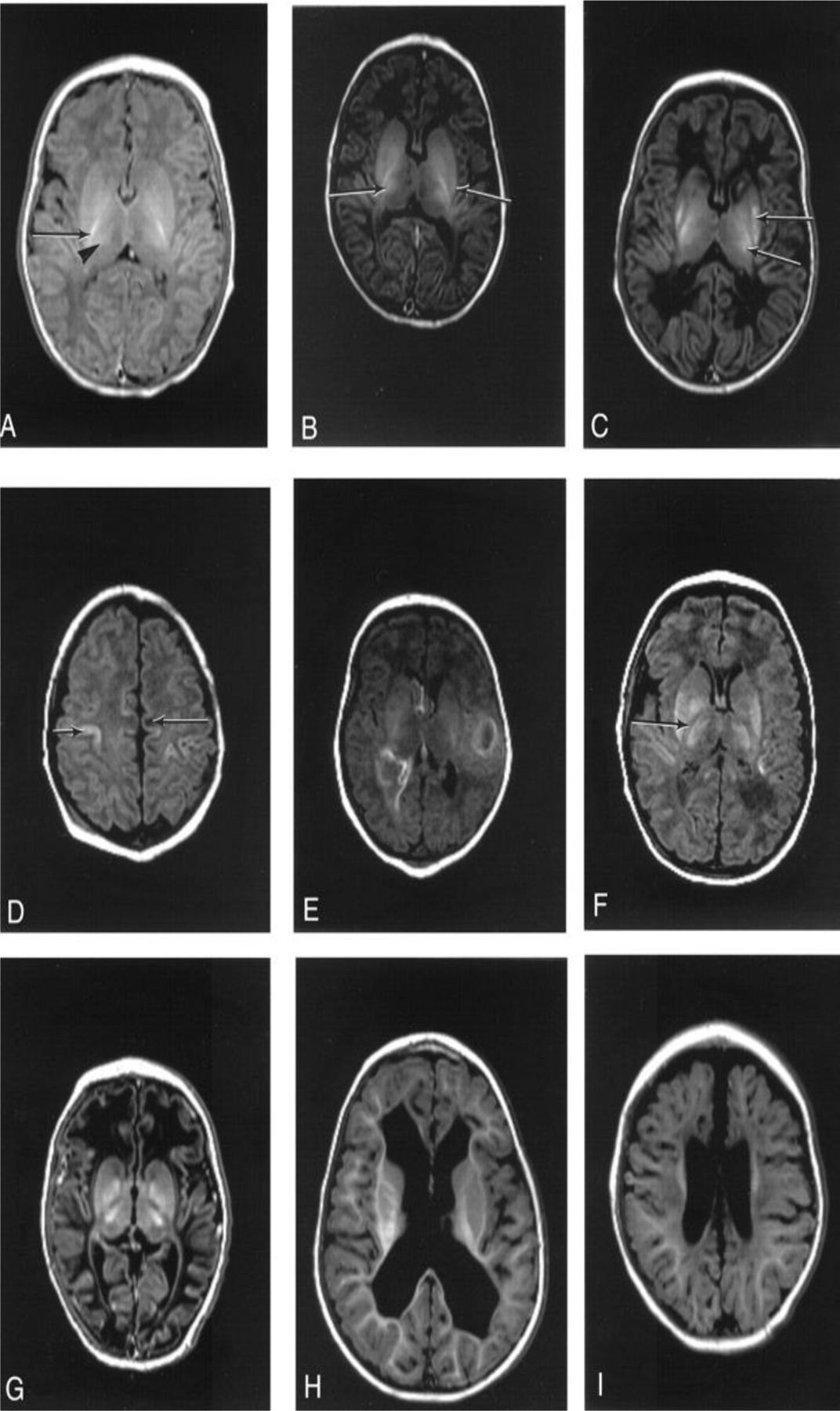
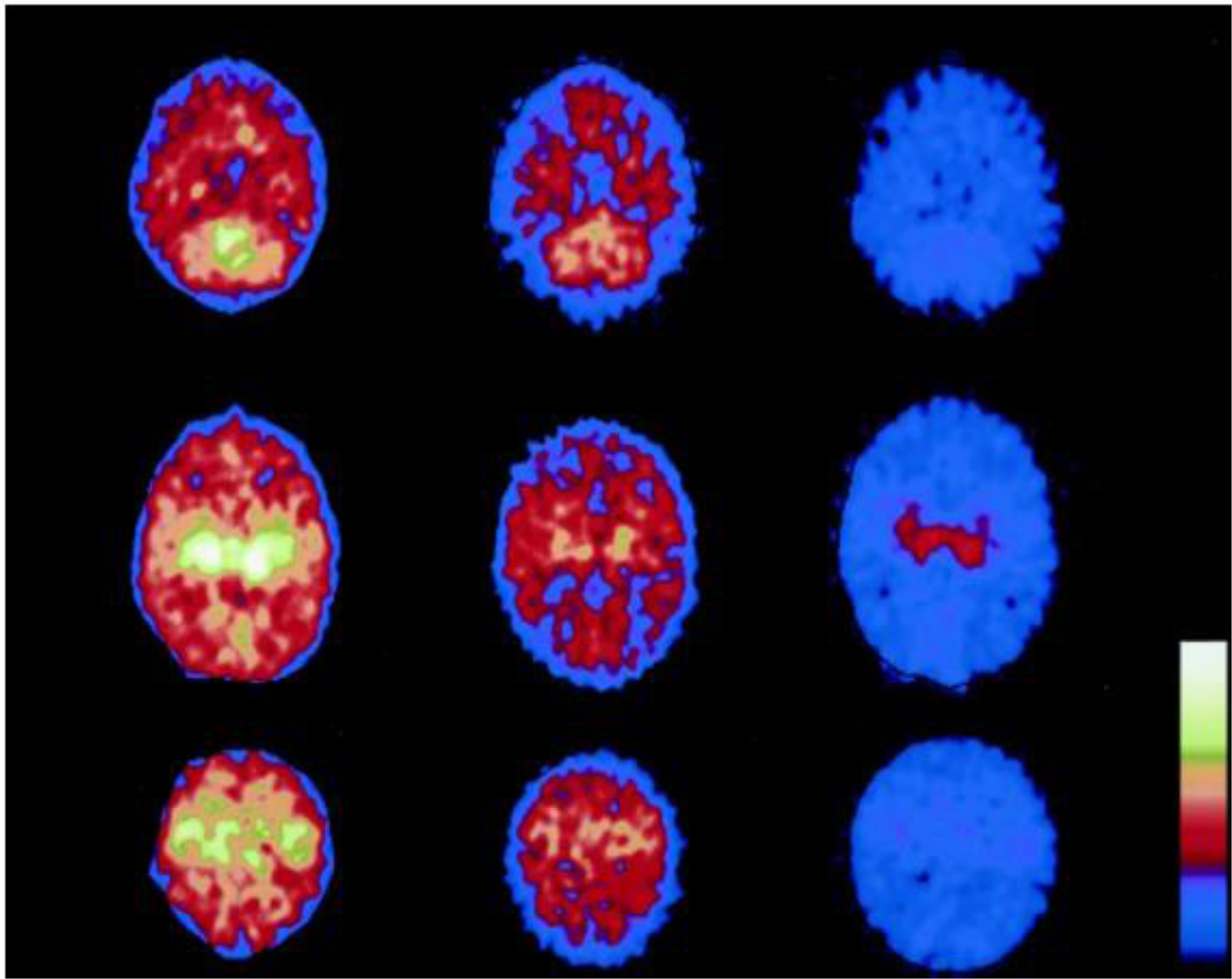
Fetal, perinatal, and neonatal asphyxia are vital health issues for the most vulnerable groups in human beings, including fetuses, newborns, and infants. Severe reduction in oxygen and blood supply to the fetal brain can cause hypoxic-ischemic encephalopathy (HIE), leading to long-term neurological disorders, including mental impairment and cerebral palsy. Such neurological disorders are major healthcare concerns. Therefore, there has been a continuous effort to develop clinically useful diagnostic tools for accurately and quantitatively measuring and monitoring blood and oxygen supply to the fetal and neonatal brain to avoid severe consequences of asphyxia HIE and neonatal encephalopathy. Major diagnostic technologies used for this purpose include fetal heart rate monitoring, fetus scalp blood sampling, ultrasound imaging, magnetic resonance imaging, X-ray computed tomography, and nuclear medicine. In addition, given the limitations and shortcomings of traditional diagnostic methods, emerging technologies such as near-infrared spectroscopy and photoacoustic imaging have also been introduced as stand-alone or complementary solutions to address this critical gap in fetal and neonatal care. This review provides a thorough overview of the traditional and emerging technologies for monitoring fetal and neonatal brain oxygenation status and describes their clinical utility, performance, advantages, and disadvantages.
Keywords: Blood flow; Diagnostic imaging; Fetal asphyxia; Hypoxic-ischemic encephalopathy; Magnetic resonance imaging; Neonatal asphyxia; Neonatal encephalopathy; Oxygenation; Photoacoustic imaging; Ultrasound; X-ray computed tomography.
© 2021 S. Karger AG, Basel.
Conflict of interest statement
Conflict of Interest Statement
Dr. Hernandez is an Editorial Board Member of Fetal Diagnosis and Therapy. The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Fifty years of brain imaging in neonatal encephalopathy following perinatal asphyxia.Pediatr Res. 2017 Jan;81(1-2):150-155. doi: 10.1038/pr.2016.195. Epub 2016 Sep 27. Pediatr Res. 2017. PMID: 27673422 Review.
-
Near-infrared spectroscopy versus magnetic resonance imaging to study brain perfusion in newborns with hypoxic-ischemic encephalopathy treated with hypothermia.Neuroimage. 2014 Jan 15;85 Pt 1(0 1):287-93. doi: 10.1016/j.neuroimage.2013.04.072. Epub 2013 Apr 28. Neuroimage. 2014. PMID: 23631990 Free PMC article.
-
[Role of cerebral computed tomography in the evaluation of brain injury following hypoxia in neonates].Zhongguo Dang Dai Er Ke Za Zhi. 2006 Jun;8(3):195-7. Zhongguo Dang Dai Er Ke Za Zhi. 2006. PMID: 16787589 Chinese.
-
[Perinatal asphyxia, hypoxic-ischemic encephalopathy and neurological sequelae in full-term newborns. II. Description and interrelation].Rev Neurol. 1996 Aug;24(132):969-76. Rev Neurol. 1996. PMID: 8755359 Spanish.
-
Neuroimaging and Other Neurodiagnostic Tests in Neonatal Encephalopathy.Clin Perinatol. 2016 Sep;43(3):511-27. doi: 10.1016/j.clp.2016.04.009. Clin Perinatol. 2016. PMID: 27524451 Review.
Cited by
-
Diagnostic potential of NRG1 in benign nerve sheath tumors and its influence on the PI3K-Akt signaling and tumor immunity.Diagn Pathol. 2024 Feb 8;19(1):28. doi: 10.1186/s13000-024-01438-9. Diagn Pathol. 2024. PMID: 38331905 Free PMC article.
-
Independent component analysis algorithms for non-invasive fetal electrocardiography.PLoS One. 2023 Jun 6;18(6):e0286858. doi: 10.1371/journal.pone.0286858. eCollection 2023. PLoS One. 2023. PMID: 37279195 Free PMC article.
-
Sensitivity analysis of transabdominal fetal pulse oximetry using MRI-based simulations.Biomed Opt Express. 2024 Aug 19;15(9):5280-5295. doi: 10.1364/BOE.531149. eCollection 2024 Sep 1. Biomed Opt Express. 2024. PMID: 39296401 Free PMC article.
-
Advanced magnetic resonance imaging in human placenta: insights into fetal growth restriction and congenital heart disease.Front Cardiovasc Med. 2024 Jul 23;11:1426593. doi: 10.3389/fcvm.2024.1426593. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39108671 Free PMC article. Review.
-
FOXP2 Expression and Oral Feeding Success in Preterm Infants: Sex 2 Differences.Genes (Basel). 2025 Feb 4;16(2):190. doi: 10.3390/genes16020190. Genes (Basel). 2025. PMID: 40004519 Free PMC article.
References
-
- Encephalopathy N, and Neurologic Outcome, “Report of the American College of Obstetricians and Gynecologists’ Task Force on neonatal encephalopathy,” Obstet Gynecol, vol. 123, no. 4, pp. 896–901, 2014. - PubMed
-
- Graham EM, Ruis KA, Hartman AL, Northington FJ, and Fox HE, “A systematic review of the role of intrapartum hypoxia-ischemia in the causation of neonatal encephalopathy,” American journal of obstetrics and gynecology, vol. 199, no. 6, pp. 587–595, 2008. - PubMed
-
- Thornberg E, Thiringer K, Odeback A, and Milsom I, “Birth asphyxia: incidence, clinical course and outcome in a Swedish population,” Acta paediatrica, vol. 84, no. 8, pp. 927–932, 1995. - PubMed
-
- Kurinczuk JJ, White-Koning M, and Badawi N, “Epidemiology of neonatal encephalopathy and hypoxic–ischaemic encephalopathy,” Early human development, vol. 86, no. 6, pp. 329–338, 2010. - PubMed
-
- Barcroft J, “The Croonian lecture-Foetal respiration,” Proceedings of the Royal Society of London. Series B-Biological Sciences, vol. 118, no. 808, pp. 242–263, 1935.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
