

Comparative analysis of long-term oncologic outcomes for minimally invasive and open Ivor Lewis esophagectomy after neoadjuvant chemoradiation: a propensity score matched observational study
- PMID: 34872562
- PMCID: PMC8647339
- DOI: 10.1186/s13019-021-01728-z
Comparative analysis of long-term oncologic outcomes for minimally invasive and open Ivor Lewis esophagectomy after neoadjuvant chemoradiation: a propensity score matched observational study
Abstract
Background: Locally advanced esophageal carcinoma is typically treated with neoadjuvant chemoradiation and esophagectomy (trimodality therapy). We compared the long-term oncologic outcomes of minimally invasive Ivor Lewis esophagectomy (M-ILE) cohort with a propensity score weighted cohort of open Ivor Lewis esophagectomy (O-ILE) cases after trimodality therapy.
Methods: This is a retrospective review of 223 patients diagnosed with esophageal carcinoma who underwent neoadjuvant chemoradiation followed by M-ILE or O-ILE from April 2009 to February 2019. Inverse probability of treatment weighting (IPTW) adjustment was used to balance the baseline characteristics between study groups. Kaplan-Meier survival curves were calculated for overall survival and recurrence-free survival comparing the two groups. Multivariate Cox proportional hazards regression models were used to determine predictive variables for overall and recurrence-free survival.
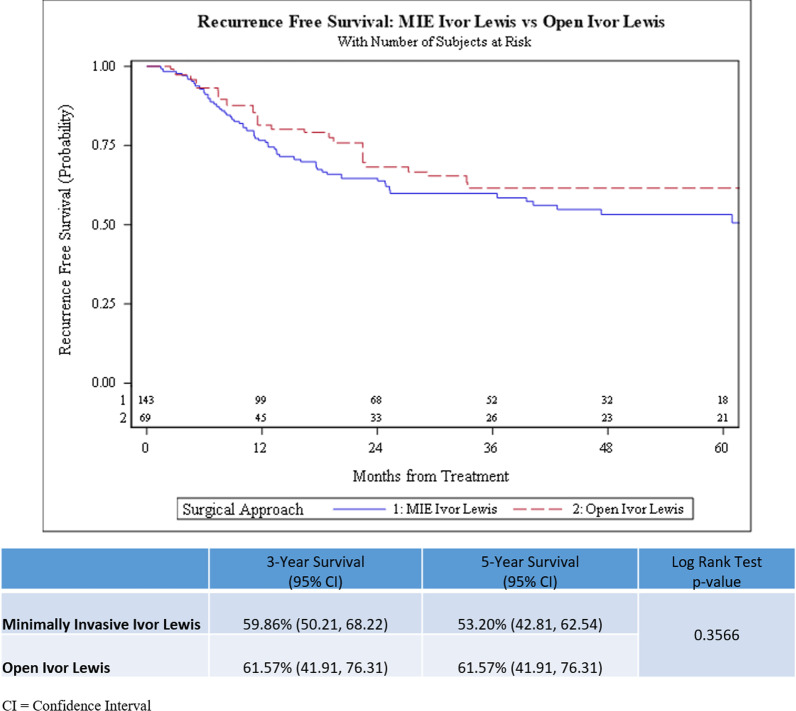
Results: The IPTW cohort included patients with esophageal carcinoma who underwent M-ILE (n = 142) or O-ILE (n = 68). The overall rate of postoperative adverse events was not significantly different after IPTW adjustment between the O-ILE and M-ILE trimodality groups (53.4% vs. 39.2%, p = 0.089). The 3-year overall survival (OS) for the M-ILE group was 59.4% (95% CI: 49.8-67.8) compared to 55.7% (95% CI: 39.2-69.4) for the O-ILE group (p = 0.670). The 3-year recurrence-free survival for the M-ILE group was 59.9% (95% CI: 50.2-68.2) compared to 61.6% (95% CI: 41.9-76.3) for the O-ILE group (p = 0.357). A complete response to neoadjuvant chemoradiation was significantly predictive of improved OS and RFS.
Conclusion: The overall and recurrence-free survival rates for M-ILE were not significantly different from O-ILE for esophageal carcinoma after trimodality therapy. Complete response to neoadjuvant chemoradiation was predictive of improved overall and recurrence- free survival.
Keywords: Esophageal carcinoma; Ivor Lewis esophagectomy; Minimally invasive esophagectomy; Neoadjuvant therapy.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests regarding the preparation of this manuscript.
Figures


Similar articles
-
An Analysis of Outcomes After Transition From Open to Minimally Invasive Ivor Lewis Esophagectomy.Ann Thorac Surg. 2021 Apr;111(4):1174-1181. doi: 10.1016/j.athoracsur.2020.06.071. Epub 2020 Sep 1. Ann Thorac Surg. 2021. PMID: 32888925
-
Neoadjuvant chemoradiation is associated with improved overall survival in older patients with esophageal cancer.J Geriatr Oncol. 2018 Jan;9(1):40-46. doi: 10.1016/j.jgo.2017.08.010. Epub 2017 Sep 6. J Geriatr Oncol. 2018. PMID: 28887066
-
Outcomes With Open and Minimally Invasive Ivor Lewis Esophagectomy After Neoadjuvant Therapy.Ann Thorac Surg. 2016 Mar;101(3):1097-103. doi: 10.1016/j.athoracsur.2015.09.062. Epub 2015 Dec 1. Ann Thorac Surg. 2016. PMID: 26652140
-
Minimally invasive and robotic Ivor Lewis esophagectomy.J Thorac Dis. 2014 May;6 Suppl 3(Suppl 3):S314-21. doi: 10.3978/j.issn.2072-1439.2014.04.32. J Thorac Dis. 2014. PMID: 24876936 Free PMC article. Review.
-
Long-term survival outcomes of esophageal cancer after minimally invasive Ivor Lewis esophagectomy.World J Surg Oncol. 2022 Feb 25;20(1):50. doi: 10.1186/s12957-022-02518-0. World J Surg Oncol. 2022. PMID: 35209914 Free PMC article. Review.
Cited by
-
Efficacy of modified thoraco-laparoscopic Ivor-Lewis versus traditional thoraco-laparoscopic Ivor-Lewis for esophageal cancer: Propensity score-matched analysis.Front Oncol. 2023 Jan 17;12:1076014. doi: 10.3389/fonc.2022.1076014. eCollection 2022. Front Oncol. 2023. PMID: 36733352 Free PMC article.
-
Minimally invasive versus open esophagectomy after neoadjuvant therapy for esophageal cancer: a meta-analysis.J Cardiothorac Surg. 2023 Mar 21;18(1):90. doi: 10.1186/s13019-023-02180-x. J Cardiothorac Surg. 2023. PMID: 36945008 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
