

A 31-Year-Old Man With Seizures, Brain Lesion, and Lung Nodules
- PMID: 34872678
- PMCID: PMC8828931
- DOI: 10.1016/j.chest.2021.07.051
A 31-Year-Old Man With Seizures, Brain Lesion, and Lung Nodules
Abstract
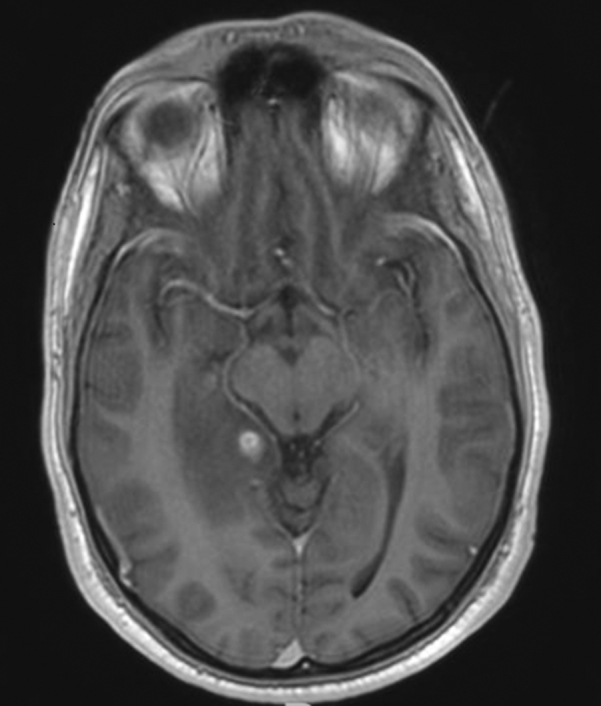
A 31-year-old man was admitted to our hospital with a recent history of generalized seizures. Three months earlier, he started with intermittent hemoptysis. CT scan showed a cavitary lung lesion in the upper segment of the right inferior lobe (RIL). Because of his job as a social worker in a high-risk population, he started treatment for Mycobacterium TB; however, the BAL culture result was negative. At the time of his current admission, he has continued taking rifampicin, isoniazid, pyrazinamide, and levofloxacin. He denied the use of any illicit drugs or alcohol. He had no history of smoking. One year earlier, he visited Southeast Asia, Oceania, and South Africa for several months. He reported a weight loss of 7 kg since then. Except for a recurrent oral candidiasis, he did not have a relevant medical history. His family history was notable for mother with lupus, and brother with sarcoidosis.
Copyright © 2021 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Response.Chest. 2022 May;161(5):e327-e328. doi: 10.1016/j.chest.2022.01.028. Chest. 2022. PMID: 35526908 No abstract available.
-
Dihydrorhodamine Test From a Clinical Point of View.Chest. 2022 May;161(5):e327. doi: 10.1016/j.chest.2022.01.027. Chest. 2022. PMID: 35526909 No abstract available.
References
-
- Bassiri-Jahromi S., Doostkam A. Fungal infection and increased mortality in patients with chronic granulomatous disease. J Mycol Med. 2012;22:52–57. - PubMed
-
- Dotis J., Pana Z.D., Roilides E. Non-Aspergillus fungal infections in chronic granulomatous disease. Mycoses. 2013;56:449–462. - PubMed
-
- Rawat A., Bhattad S., Singh S. Chronic granulomatous disease. Indian J Pediatr. 2016;83:345–353. - PubMed
-
- Thomsen I.P., Smith M.A., Holland S.M., Creech C.B. A comprehensive approach to the management of children and adults with chronic granulomatous disease. J Allergy Clin Immunol Pract. 2016;4:1082–1088. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
