

Collaborative Heart Attack Management Program (CHAMP): use of prehospital thrombolytics to improve timeliness of STEMI management in British Columbia
- PMID: 34872989
- PMCID: PMC8650474
- DOI: 10.1136/bmjoq-2021-001519
Collaborative Heart Attack Management Program (CHAMP): use of prehospital thrombolytics to improve timeliness of STEMI management in British Columbia
Abstract
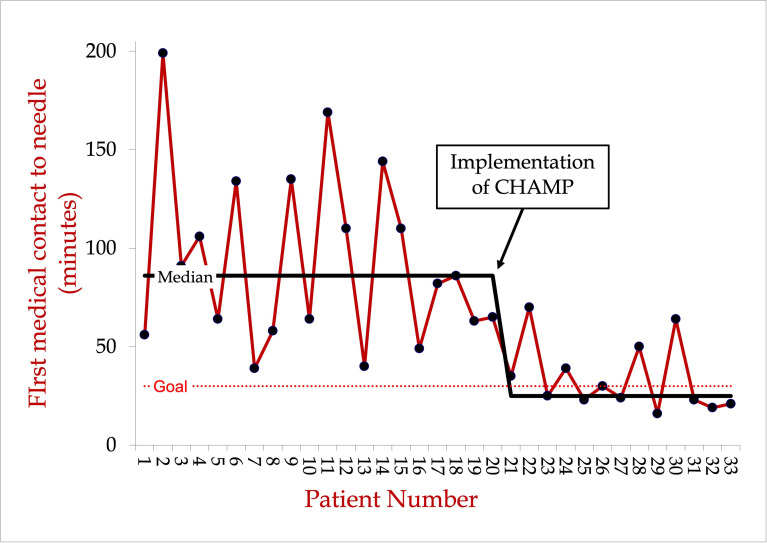
Coronary artery disease is the second leading cause of death in Canada. Time to treatment in ST-elevation myocardial infarction (STEMI) is directly related to morbidity and mortality. Thrombolysis is the primary treatment for STEMI in many regions of Canada because of prolonged transport times to percutaneous coronary intervention-capable centres. To reduce time from first medical contact (FMC) to thrombolysis, some emergency medical services (EMS) systems have implemented prehospital thrombolysis (PHT). PHT is not a novel concept and has a strong evidence base showing reduced mortality.Here, we describe a quality improvement initiative to decrease time from FMC to thrombolysis using PHT and aim to describe our methods and challenges during implementation. We used a quality improvement framework to collaborate with hospitals, EMS, cardiology, emergency medicine and other stakeholders during implementation. We trained advanced care paramedics to administer thrombolysis in STEMI with remote cardiologist support and aimed to achieve a guideline-recommended median FMC to needle time of <30 min in 80% of patients.Overall, we reduced our median FMC to needle time by 70%. Our baseline patients undergoing in-hospital thrombolysis had a median time of 84 min (IQR 62-116 min), while patients after implementation of PHT had a median time of 25 min (IQR 23-39 min). Patients treated within the guideline-recommended time from FMC to needle of <30 min increased from 0% at baseline to 61% with PHT. Return on investment analysis showed $2.80 saved in acute care costs for every $1.00 spent on the intervention.While we did not achieve our goal of 80% compliance with FMC to needle time of <30 min, our results show that the intervention substantially reduced the FMC to needle time and overall cost. We plan to continue with ongoing implementation of PHT through expansion to other communities in our province.
Keywords: ST elevation myocardial infarction; emergency medical services; fibrinolysis; quality improvement.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Statistics Canada . Table 13-10-0394-01 leading causes of death, total population, by age group, 2020. P. 1
-
- Goel K, Pinto DS, Gibson CM. Association of time to reperfusion with left ventricular function and heart failure in patients with acute myocardial infarction treated with primary percutaneous coronary intervention: a systematic review. Am Heart J 2013;165:451–67. 10.1016/j.ahj.2012.11.014 - DOI - PubMed
-
- Scholz KH, Maier SKG, Maier LS, et al. Impact of treatment delay on mortality in ST-segment elevation myocardial infarction (STEMI) patients presenting with and without haemodynamic instability: results from the German prospective, multicentre FITT-STEMI trial. Eur Heart J 2018;39:1065–74. 10.1093/eurheartj/ehy004 - DOI - PMC - PubMed
-
- Wong GC, Welsford M, Ainsworth C, et al. 2019 Canadian cardiovascular Society/Canadian association of interventional cardiology guidelines on the acute management of ST-elevation myocardial infarction: focused update on regionalization and reperfusion. Can J Cardiol 2019;35:107–32. 10.1016/j.cjca.2018.11.031 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical