

Transcatheter aortic valve implantation versus surgical aortic valve replacement in patients with severe aortic stenosis: a systematic review and meta-analysis
- PMID: 34873012
- PMCID: PMC8650468
- DOI: 10.1136/bmjopen-2021-054222
Transcatheter aortic valve implantation versus surgical aortic valve replacement in patients with severe aortic stenosis: a systematic review and meta-analysis
Abstract
Objectives: Patients undergoing surgery for severe aortic stenosis (SAS) can be treated with either transcatheter aortic valve implantation (TAVI) or surgical aortic valve replacement (SAVR). The choice of procedure depends on several factors, including the clinical judgement of the heart team and patient preferences, which are captured by actively informing and involving patients in a process of shared decision making (SDM). We synthesised the most up-to-date and accessible evidence on the benefits and risks that may be associated with TAVI versus SAVR to support SDM in this highly personalised decision-making process.
Design: Systematic review and meta-analysis.
Data sources: MEDLINE (Ovid), Embase (Ovid) and the Cochrane Central Register of Controlled Trials (CENTRAL; Wiley) were searched from January 2000 to August 2020 with no language restrictions. Reference lists of included studies were searched to identify additional studies.
Eligibility criteria: Randomised controlled trials (RCTs) that compared TAVI versus SAVR in patients with SAS and reported on all-cause or cardiovascular mortality, length of stay in intensive care unit or hospital, valve durability, rehospitalisation/reintervention, stroke (any stroke or major/disabling stroke), myocardial infarction, major vascular complications, major bleeding, permanent pacemaker (PPM) implantation, new-onset or worsening atrial fibrillation (NOW-AF), endocarditis, acute kidney injury (AKI), recovery time or pain were included.
Data extraction and synthesis: Two independent reviewers were involved in data extraction and risk of bias (ROB) assessment using the Cochrane tool (one reviewer extracted/assessed the data, and the second reviewer checked it). Dichotomous data were pooled using the Mantel-Haenszel method with random-effects to generate a risk ratio (RR) with 95% CI. Continuous data were pooled using the inverse-variance method with random-effects and expressed as a mean difference (MD) with 95% CI. Heterogeneity was assessed using the I2 statistic.
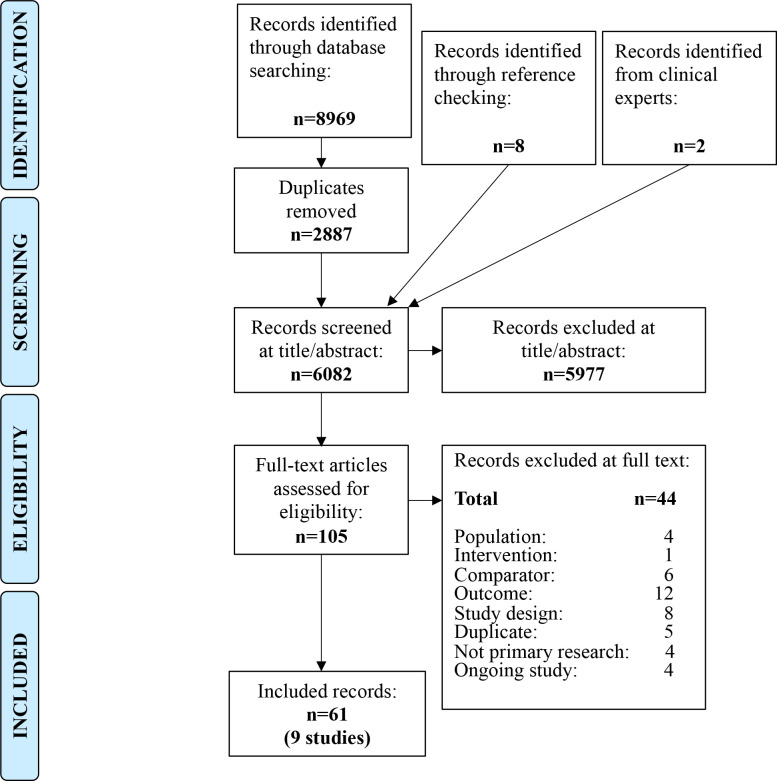
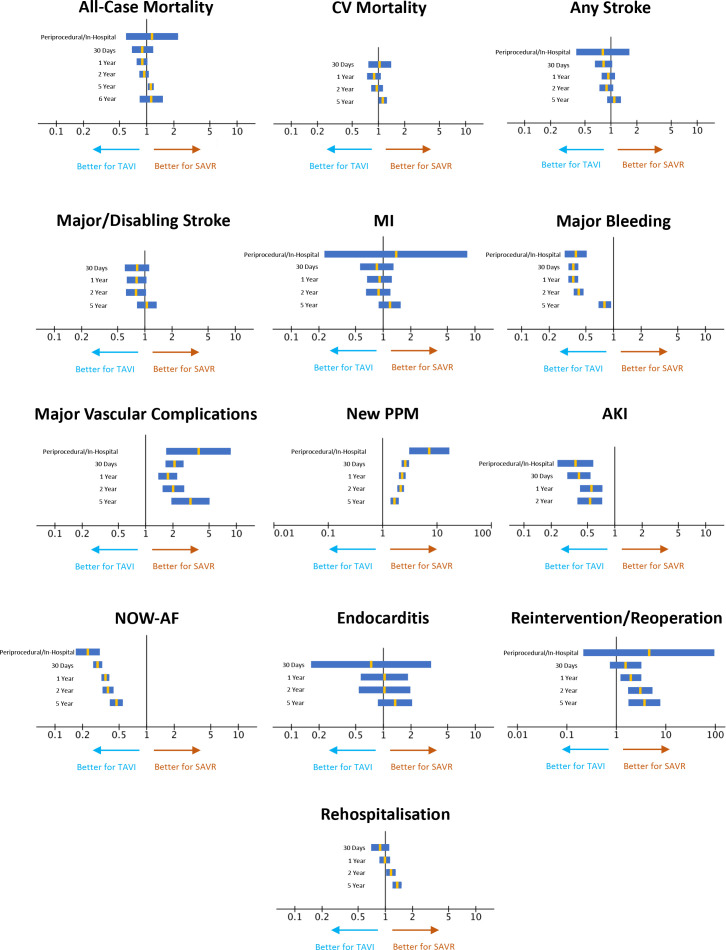
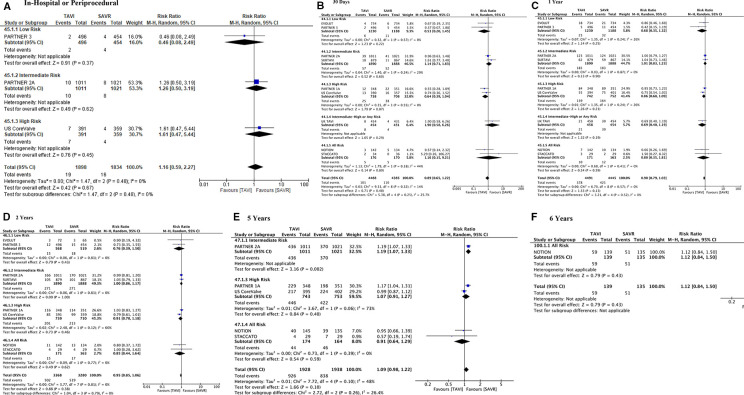
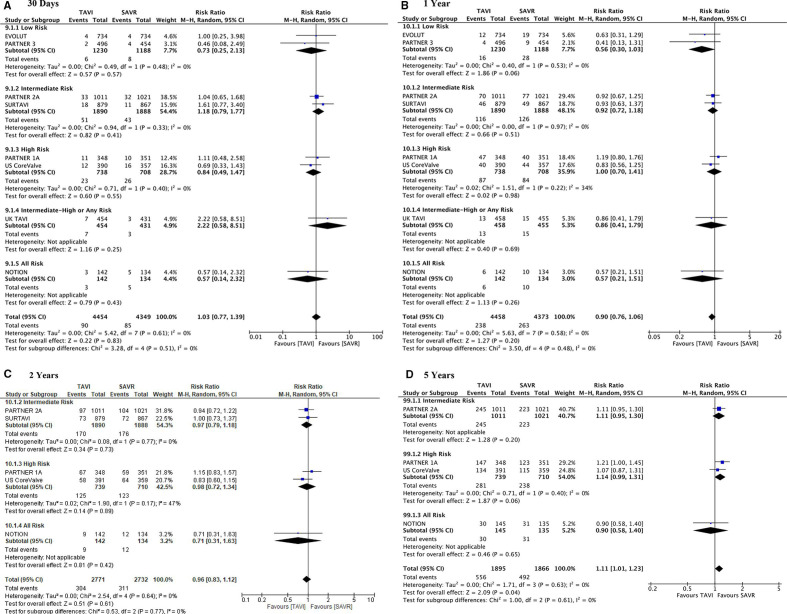
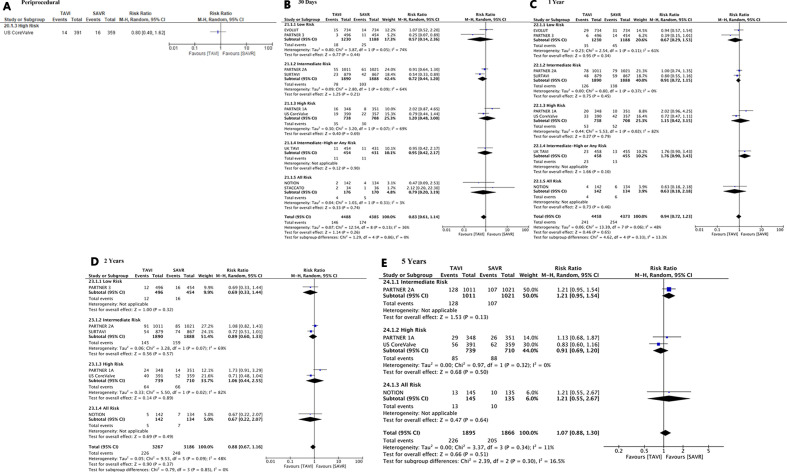
Results: 8969 records were retrieved and nine RCTs (61 records) were ultimately included (n=8818 participants). Two RCTs recruited high-risk patients, two RCTs recruited intermediate-risk patients, two RCTs recruited low-risk patients, one RCT recruited high-risk (≥70 years) or any-risk (≥80 years) patients; and two RCTs recruited all-risk or 'operable' patients. While there was no overall change in the risk of dying from any cause (30 day: RR 0.89, 95% CI 0.65 to 1.22; ≤1 year: RR 0.90, 95% CI 0.79 to 1.03; 5 years: RR 1.09, 95% CI 0.98 to 1.22), cardiovascular mortality (30 day: RR 1.03, 95% CI 0.77 to 1.39; ≤1 year: RR 0.90, 95% CI 0.76 to 1.06; 2 years: RR 0.96, 95% CI 0.83 to 1.12), or any type of stroke (30 day: RR 0.83, 95% CI 0.61 to 1.14;≤1 year: RR 0.94, 95% CI 0.72 to 1.23; 5 years: RR 1.07, 95% CI 0.88 to 1.30), the risk of several clinical outcomes was significantly decreased (major bleeding, AKI, NOW-AF) or significantly increased (major vascular complications, PPM implantation) for TAVI vs SAVR. TAVI was associated with a significantly shorter hospital stay vs SAVR (MD -3.08 days, 95% CI -4.86 to -1.29; 4 RCTs, n=2758 participants). Subgroup analysis generally favoured TAVI patients receiving implantation via the transfemoral (TF) route (vs non-TF); receiving a balloon-expandable (vs self-expanding) valve; and those at low-intermediate risk (vs high risk). All RCTs were rated at high ROB, predominantly due to lack of blinding and selective reporting.
Conclusions: No overall change in the risk of death from any cause or cardiovascular mortality was identified but 95% CIs were often wide, indicating uncertainty. TAVI may reduce the risk of certain side effects while SAVR may reduce the risk of others. Most long-term (5-year) results are limited to older patients at high surgical risk (ie, early trials), therefore more data are required for low risk populations. Ultimately, neither surgical technique was considered dominant, and these results suggest that every patient with SAS should be individually engaged in SDM to make evidence-based, personalised decisions around their care based on the various benefits and risks associated with each treatment.
Prospero registration number: CRD42019138171.
Keywords: adult cardiology; coronary intervention; valvular heart disease.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: SLS, KM, SHL, CF, JK and RW are employees of KSR, which received financial support from University Medical Center Schleswig-Holstein in connection with the development of this manuscript; they have no other conflicts of interest. TP, MD, AH, HS, JC and KW have no conflicts of interest. FS is managing partner of the SHARE TO CARE. CK and DF are consultants for Medtronic Inc. and Edwards Lifesciences, DF has received speaker’s honoraria as well as travel support. NF is a consultant for Edwards Lifesciences. GL is a consultant for Abbott.
Figures
References
-
- Aortic Stenosis Writing Group, Bonow RO, Brown AS, et al. . ACC/AATS/AHA/ASE/EACTS/HVS/SCA/SCAI/SCCT/SCMR/STS 2017 appropriate use criteria for the treatment of patients with severe aortic stenosis: a report of the American College of cardiology appropriate use criteria Task force, American association for thoracic surgery, American heart association, American Society of echocardiography, European association for Cardio-Thoracic surgery, heart valve Society, society of cardiovascular Anesthesiologists, Society for cardiovascular angiography and interventions, society of cardiovascular computed tomography, Society for cardiovascular magnetic resonance, and society of thoracic surgeons. J Am Soc Echocardiogr 2018;31:117–47. 10.1016/j.echo.2017.10.020 - DOI - PubMed
-
- Kuck K-H, Eggebrecht H, Elsässer A. Qualitätskriterien Zur Durchführung Der kathetergestützten Aortenklappenimplantation (TAVI): Aktualisierung des Positionspapiers Der Deutschen Gesellschaft für Kardiologie. Berlin: Springer-Verlag, 2016.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous