

Antibiotics in critically ill children-a narrative review on different aspects of a rational approach
- PMID: 34873285
- PMCID: PMC8816725
- DOI: 10.1038/s41390-021-01878-9
Antibiotics in critically ill children-a narrative review on different aspects of a rational approach
Abstract
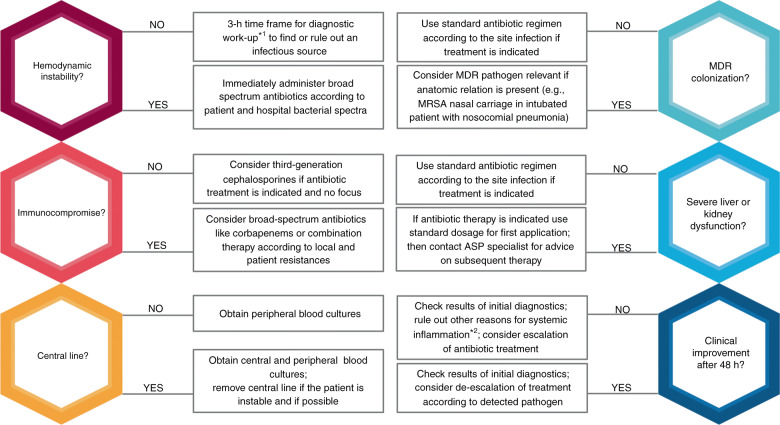
Especially critically ill children are exposed to antibiotic overtreatment, mainly caused by the fear of missing out a severe bacterial infection. Potential adverse effects and selection of multi-drug resistant bacteria play minor roles in decision making. This narrative review first describes harm from antibiotics and second focuses on different aspects that could help to reduce antibiotic overtreatment without harming the patient: harm from antibiotic treatment, diagnostic approaches, role of biomarkers, timing of antibiotic therapy, empiric therapy, targeted therapy, and therapeutic drug monitoring. Wherever possible, we linked the described evidence to the current Surviving Sepsis Campaign guidelines. Antibiotic stewardship programs should help guiding antibiotic therapy for critically ill children. IMPACT: Critically ill children can be harmed by inadequate or overuse of antibiotics. Hemodynamically unstable children with a suspicion of infection should be immediately treated with broad-spectrum antibiotics. In contrast, in hemodynamically stable children with sepsis and organ dysfunction, a time frame of 3 h for proper diagnostics may be adequate before starting antibiotics if necessary. Less and more targeted antibiotic treatment can be achieved via antibiotic stewardship programs.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Optimal and responsible use of antibiotics.Curr Opin Crit Care. 2019 Oct;25(5):458-464. doi: 10.1097/MCC.0000000000000645. Curr Opin Crit Care. 2019. PMID: 31369410 Review.
-
Antibiotic stewardship in sepsis management: toward a balanced use of antibiotics for the severely ill patient.Expert Rev Anti Infect Ther. 2019 Feb;17(2):89-97. doi: 10.1080/14787210.2019.1568239. Epub 2019 Jan 23. Expert Rev Anti Infect Ther. 2019. PMID: 30672354 Review.
-
Ineffectiveness of procalcitonin-guided antibiotic therapy in severely critically ill patients: A meta-analysis.Int J Infect Dis. 2019 Aug;85:158-166. doi: 10.1016/j.ijid.2019.05.034. Epub 2019 Jun 21. Int J Infect Dis. 2019. PMID: 31229612
-
Antibiotic therapy in sepsis: No next time for a second chance!J Clin Pharm Ther. 2021 Aug;46(4):872-876. doi: 10.1111/jcpt.13403. Epub 2021 Mar 12. J Clin Pharm Ther. 2021. PMID: 33710622
-
Prevalence of Antibiotic-Resistant Pathogens in Culture-Proven Sepsis and Outcomes Associated With Inadequate and Broad-Spectrum Empiric Antibiotic Use.JAMA Netw Open. 2020 Apr 1;3(4):e202899. doi: 10.1001/jamanetworkopen.2020.2899. JAMA Netw Open. 2020. PMID: 32297949 Free PMC article.
Cited by
-
Retrospective analysis of 300 microbial cell-free DNA sequencing results in routine blood stream infection diagnostics.Front Cell Infect Microbiol. 2025 Jan 30;15:1504262. doi: 10.3389/fcimb.2025.1504262. eCollection 2025. Front Cell Infect Microbiol. 2025. PMID: 39949721 Free PMC article.
-
In Vitro Effects of Some Antibiotics on Purified β-Glucosidases from Rat Liver and Kidney Tissues.Antibiotics (Basel). 2025 May 30;14(6):563. doi: 10.3390/antibiotics14060563. Antibiotics (Basel). 2025. PMID: 40558153 Free PMC article.
-
Update on Therapeutic Drug Monitoring of Beta-Lactam Antibiotics in Critically Ill Patients-A Narrative Review.Antibiotics (Basel). 2023 Mar 13;12(3):568. doi: 10.3390/antibiotics12030568. Antibiotics (Basel). 2023. PMID: 36978435 Free PMC article. Review.
-
Social Determinants of Health and Antibiotic Consumption.Antibiotics (Basel). 2025 May 15;14(5):513. doi: 10.3390/antibiotics14050513. Antibiotics (Basel). 2025. PMID: 40426579 Free PMC article.
-
Paediatric and neonatal sepsis and inflammation.Pediatr Res. 2022 Jan;91(2):267-269. doi: 10.1038/s41390-021-01918-4. Epub 2022 Jan 19. Pediatr Res. 2022. PMID: 35046541 Free PMC article.
References
-
- Schlapbach LJ, et al. Mortality related to invasive infections, sepsis, and septic shock in critically ill children in Australia and New Zealand, 2002-13: a multicentre retrospective cohort study. Lancet Infect. Dis. 2015;15:46–54. - PubMed
-
- Folgori L, et al. Epidemiology and clinical outcomes of multidrug-resistant, gram-negative bloodstream infections in a European tertiary pediatric hospital during a 12-month period. Pediatr. Infect. Dis. J. 2014;33:929–932. - PubMed
-
- Noël KC, et al. International survey on determinants of antibiotic duration and discontinuation in pediatric critically Ill patients. Pediatr. Crit. Care Med. 2020;21:e696–e706. - PubMed
-
- Blinova E, et al. Point prevalence survey of antimicrobial utilization in the cardiac and pediatric critical care unit. Pediatr. Crit. Care Med. 2013;14:e280–e288. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
