

Reinfection with new variants of SARS-CoV-2 after natural infection: a prospective observational cohort in 13 care homes in England
- PMID: 34873592
- PMCID: PMC8635459
- DOI: 10.1016/S2666-7568(21)00253-1
Reinfection with new variants of SARS-CoV-2 after natural infection: a prospective observational cohort in 13 care homes in England
Abstract
Background: Understanding the duration of protection and risk of reinfection after natural infection is crucial to planning COVID-19 vaccination for at-risk groups, including care home residents, particularly with the emergence of more transmissible variants. We report on the duration, neutralising activity, and protection against the alpha variant of previous SARS-CoV-2 infection in care home residents and staff infected more than 6 months previously.
Methods: We did this prospective observational cohort surveillance in 13 care homes in Greater London, England. All staff and residents were included. Staff and residents had regular nose and throat screening for SARS-CoV-2 by RT-PCR according to national guidelines, with ad hoc testing of symptomatic individuals. From January, 2021, antigen lateral flow devices were also used, but positive tests still required RT-PCR confirmation. Staff members took the swab samples for themselves and the residents. The primary outcome was SARS-CoV-2 RT-PCR positive primary infection or reinfection in previously infected individuals, as determined by previous serological testing and screening or diagnostic RT-PCR results. Poisson regression and Cox proportional hazards models were used to estimate protective effectiveness of previous exposure. SARS-CoV-2 spike, nucleoprotein, and neutralising antibodies were assessed at multiple timepoints as part of the longitudinal follow-up.
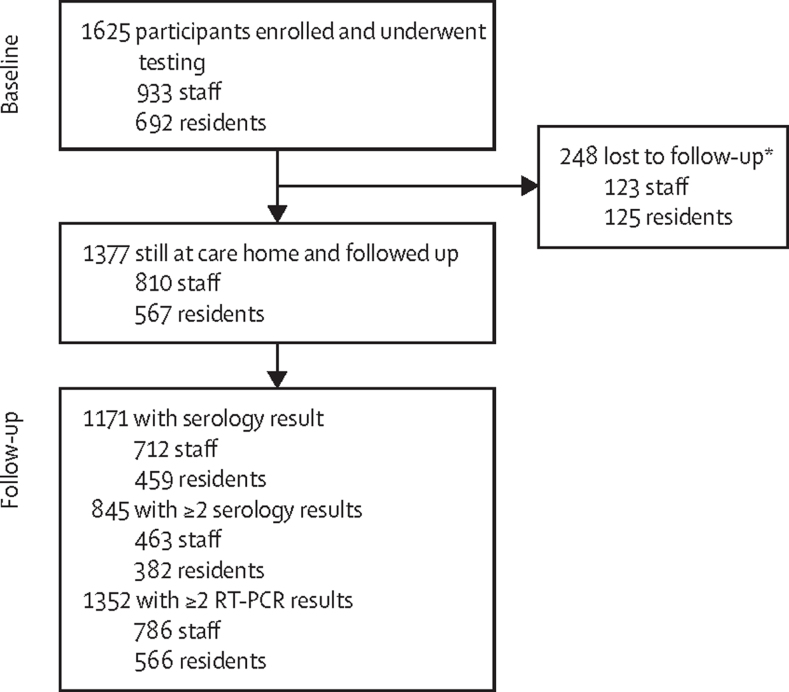
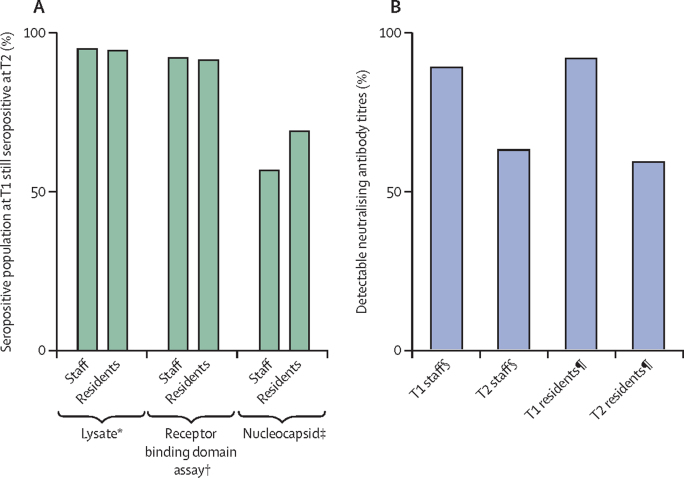
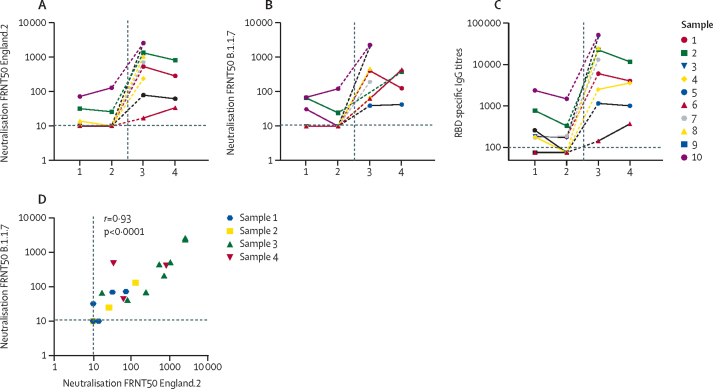
Findings: Between April 10 and Aug 3, 2020, we recruited and tested 1625 individuals (933 staff and 692 residents). 248 participants were lost to follow-up (123 staff and 125 residents) and 1377 participants were included in the follow-up period to Jan 31, 2021 (810 staff and 567 residents). There were 23 reinfections (ten confirmed, eight probable, five possible) in 656 previously infected individuals (366 staff and 290 residents), compared with 165 primary infections in 721 susceptible individuals (444 staff and 277 residents). Those with confirmed reinfections had no or low neutralising antibody concentration before reinfection, with boosting of titres after reinfection. Kinetics of binding and neutralising antibodies were similar in older residents and younger staff.
Interpretation: SARS-CoV-2 reinfections were rare in older residents and younger staff. Protection from SARS-CoV-2 was sustained for longer than 9 months, including against the alpha variant. Reinfection was associated with no or low neutralising antibody before reinfection, but significant boosting occurred on reinfection.
Funding: Public Health England.
© 2021 Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license.
Conflict of interest statement
We declare no competing interests. The authors are all employed by Public Health England, which is a public body and an executive agency of the Department of Health and Social Care.
Figures

Comment in
-
SARS-Cov-2 immune waning and reinfection in care-home settings.Lancet Healthy Longev. 2021 Dec;2(12):e776-e777. doi: 10.1016/S2666-7568(21)00276-2. Epub 2021 Dec 1. Lancet Healthy Longev. 2021. PMID: 34873591 Free PMC article. No abstract available.
References
-
- Office for National Statistics Coronavirus (COVID-19) related deaths by occupation, England and Wales: deaths registered between 9 March and 28 December 2020. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/...
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
