

Advances in liver US, CT, and MRI: moving toward the future
- PMID: 34873633
- PMCID: PMC8648935
- DOI: 10.1186/s41747-021-00250-0
Advances in liver US, CT, and MRI: moving toward the future
Abstract
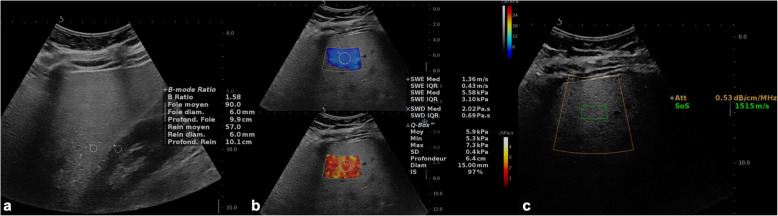
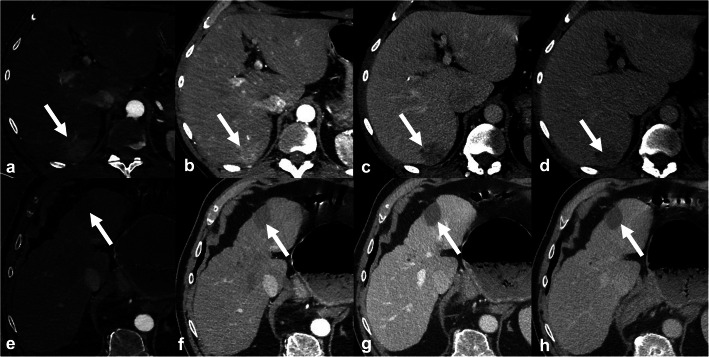
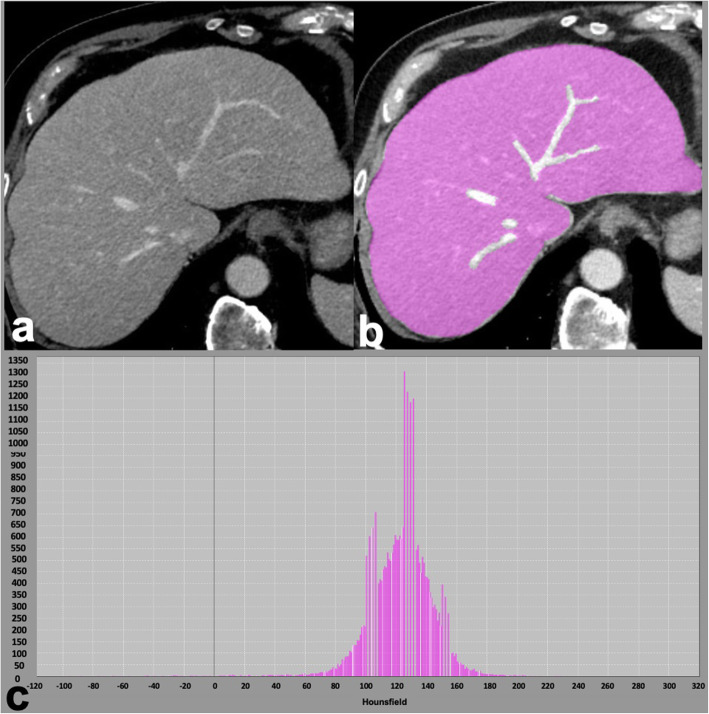
Over the past two decades, the epidemiology of chronic liver disease has changed with an increase in the prevalence of nonalcoholic fatty liver disease in parallel to the advent of curative treatments for hepatitis C. Recent developments provided new tools for diagnosis and monitoring of liver diseases based on ultrasound (US), computed tomography (CT), and magnetic resonance imaging (MRI), as applied for assessing steatosis, fibrosis, and focal lesions. This narrative review aims to discuss the emerging approaches for qualitative and quantitative liver imaging, focusing on those expected to become adopted in clinical practice in the next 5 to 10 years. While radiomics is an emerging tool for many of these applications, dedicated techniques have been investigated for US (controlled attenuation parameter, backscatter coefficient, elastography methods such as point shear wave elastography [pSWE] and transient elastography [TE], novel Doppler techniques, and three-dimensional contrast-enhanced ultrasound [3D-CEUS]), CT (dual-energy, spectral photon counting, extracellular volume fraction, perfusion, and surface nodularity), and MRI (proton density fat fraction [PDFF], elastography [MRE], contrast enhancement index, relative enhancement, T1 mapping on the hepatobiliary phase, perfusion). Concurrently, the advent of abbreviated MRI protocols will help fulfill an increasing number of examination requests in an era of healthcare resource constraints.
Keywords: Biomarkers; Magnetic resonance imaging; Non-alcoholic fatty liver disease; Tomography; Ultrasonography; X-ray computed.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures






References
-
- Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, George J, Bugianesi E. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15:11–20. - PubMed
-
- Lombardi A, Mondelli MU, ESCMID Study Group for Viral Hepatitis (ESGVH) Hepatitis C: is eradication possible? Liver Int. 2019;39:416–426. - PubMed
-
- Kleiner DE, Brunt EM, Van Natta M, et al. Nonalcoholic Steatohepatitis Clinical Research Network. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41:1313–1321. - PubMed
-
- Byrne CD, Targher G. NAFLD: a multisystem disease. J Hepatol. 2015;62:S47–S64. - PubMed
-
- Ratziu V, Charlotte F, Heurtier A, Gombert S, Giral P, Bruckert E, Grimaldi A, Capron F, Poynard T, LIDO Study Group Sampling variability of liver biopsy in nonalcoholic fatty liver disease. Gastroenterology. 2005;128:1898–1906. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous