

Validation of the portable virtual reality training system for robotic surgery (PoLaRS): a randomized controlled trial
- PMID: 34873652
- PMCID: PMC9160149
- DOI: 10.1007/s00464-021-08906-z
Validation of the portable virtual reality training system for robotic surgery (PoLaRS): a randomized controlled trial
Abstract
Background: As global use of surgical robotic systems is steadily increasing, surgical simulation can be an excellent way for robotic surgeons to acquire and retain their skills in a safe environment. To address the need for training in less wealthy parts of the world, an affordable surgical robot simulator (PoLaRS) was designed.
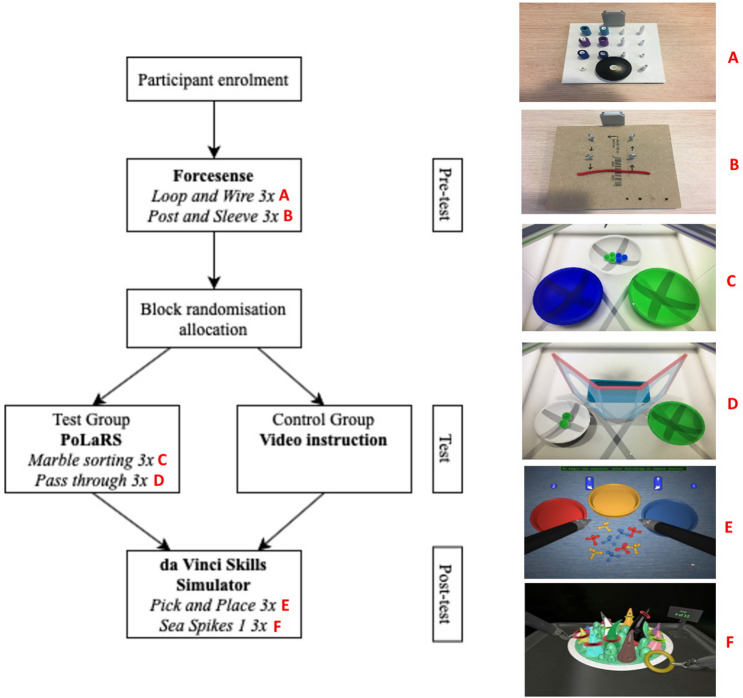
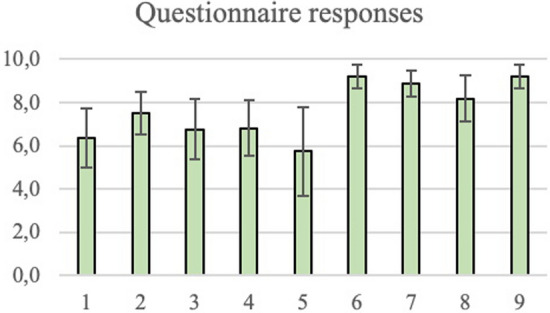
Methods: The aim of this pilot study is to compare learning curve data of the PoLaRS prototype with those of Intuitive Surgical's da Vinci Skills Simulator (dVSS) and to establish face- and construct validity. Medical students were divided into two groups; the test group (n = 18) performing tasks on PoLaRS and dVSS, and the control group (n = 20) only performing tasks on the dVSS. The performance parameters were Time, Path length, and the number of collisions. Afterwards, the test group participants filled in a questionnaire regarding both systems.
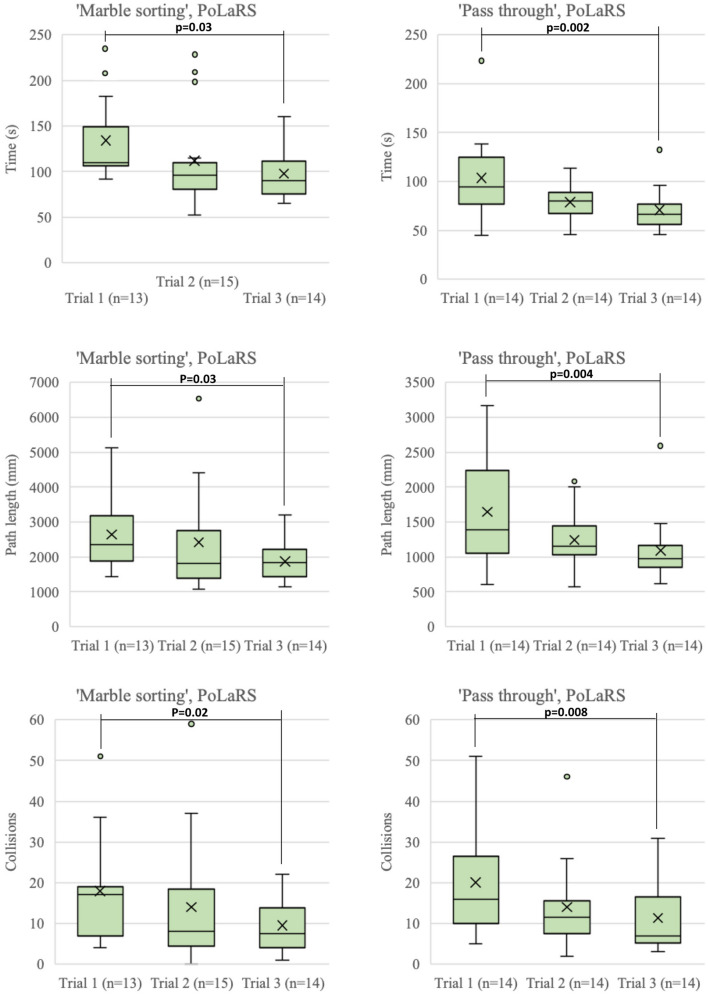
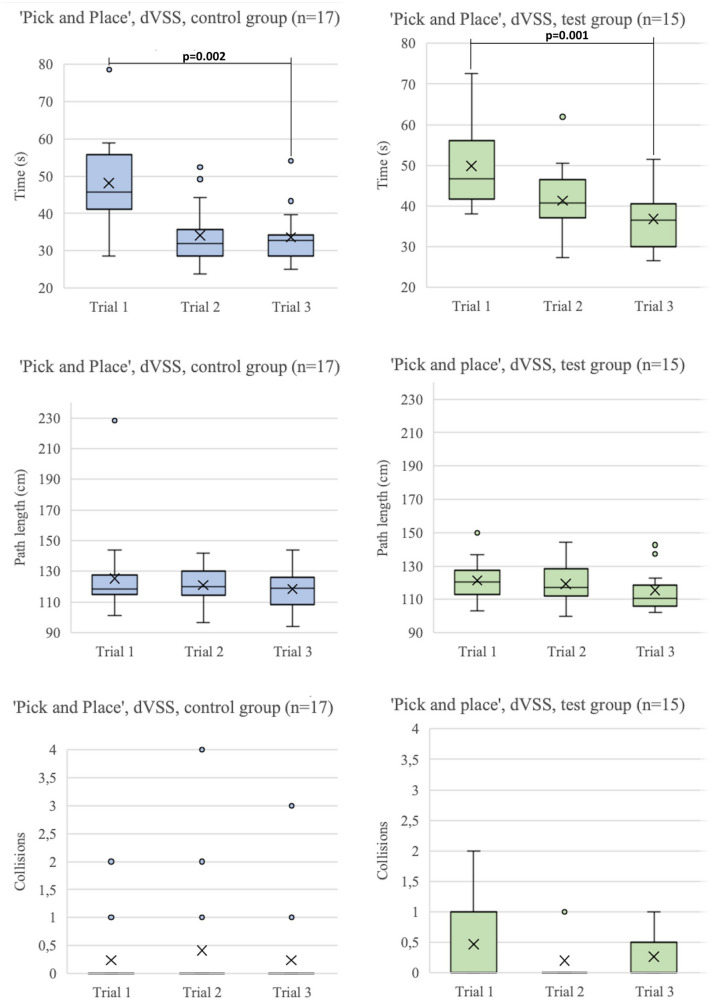
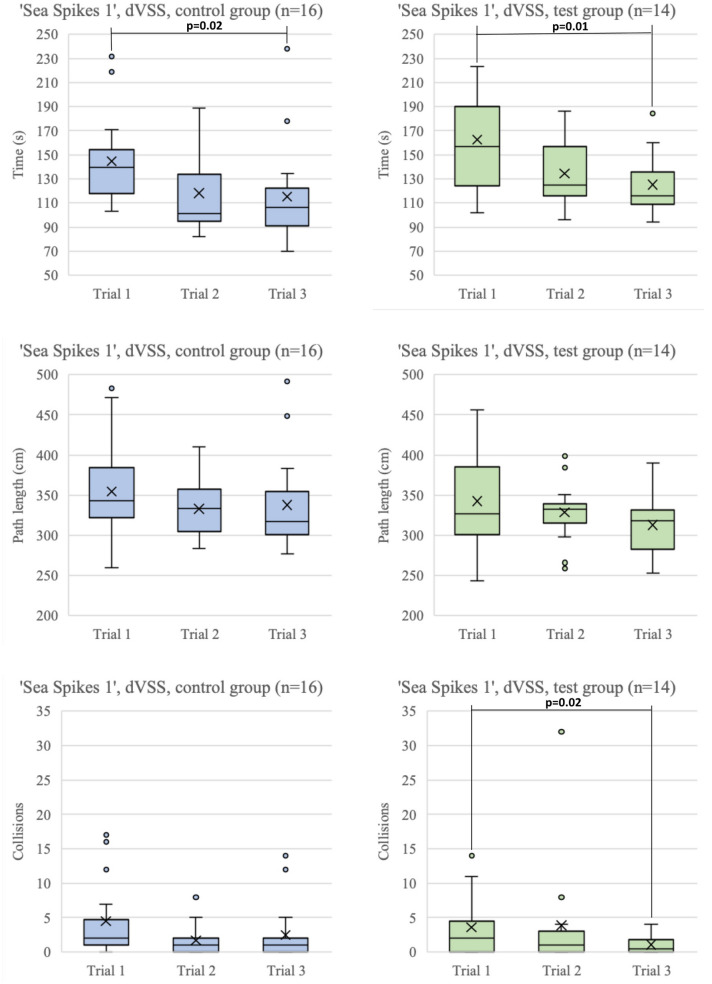
Results: A total of 528 trials executed by 38 participants were measured and included for analyses. The test group significantly improved in Time, Path Length and Collisions during the PoLaRS test phase (P ≤ 0.028). No differences was found between the test group and the control group in the dVSS performances during the post-test phase. Learning curves showed similar shapes between both systems, and between both groups. Participants recognized the potential benefits of simulation training on the PoLaRS system.
Conclusions: Robotic surgical skills improved during training with PoLaRS. This shows the potential of PoLaRS to become an affordable alternative to current surgical robot simulators. Validation with similar tasks and different expert levels is needed before implementing the training system into robotic training curricula.
Keywords: Learning curve; Patient safety-LMIC; Robot surgery; Simulation training.
© 2021. The Author(s).
Conflict of interest statement
Tim Horeman is founder of the Medtech start-up company Surge-On Medical that collaborated in the development of PolaRS. Sem F. Hardon, Anton Kooijmans, Roel Horeman, Maarten van der Elst and Alexander L.A. Bloemendaal have no conflicts of interest or financial ties to disclose.
Figures

References
-
- Surgical robots market size, share and industry analysis by application (General Surgery, Gynecology, Urology Orthopedics, Others) and regional forecast, 2019–2026. Market Research Report, July 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
