

Ambulatory electrocardiographic markers predict serious cardiac events in patients with chronic kidney disease: The Japanese Noninvasive Electrocardiographic Risk Stratification of Sudden Cardiac Death in Chronic Kidney Disease (JANIES-CKD) study
- PMID: 34873791
- PMCID: PMC8916573
- DOI: 10.1111/anec.12923
Ambulatory electrocardiographic markers predict serious cardiac events in patients with chronic kidney disease: The Japanese Noninvasive Electrocardiographic Risk Stratification of Sudden Cardiac Death in Chronic Kidney Disease (JANIES-CKD) study
Abstract
Background: Noninvasive electrocardiographic markers (NIEMs) are promising arrhythmic risk stratification tools for assessing the risk of sudden cardiac death. However, little is known about their utility in patients with chronic kidney disease (CKD) and organic heart disease. This study aimed to determine whether NIEMs can predict cardiac events in patients with CKD and structural heart disease (CKD-SHD).
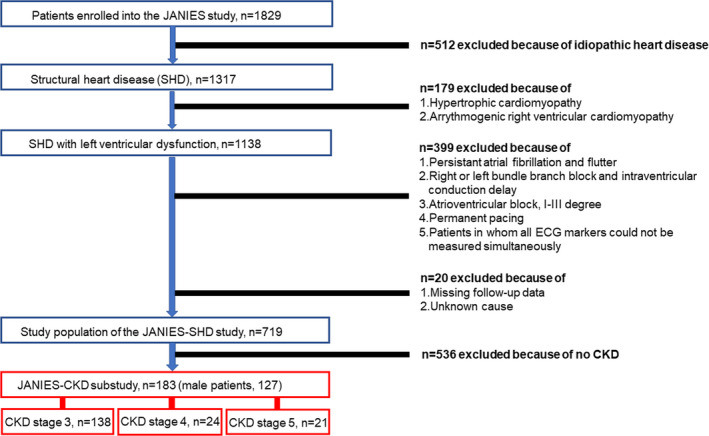
Methods: We prospectively analyzed 183 CKD-SHD patients (median age, 69 years [interquartile range, 61-77 years]) who underwent 24-h ambulatory electrocardiographic monitoring and assessed the worst values for ambulatory-based late potentials (w-LPs), heart rate turbulence, and nonsustained ventricular tachycardia (NSVT). The primary endpoint was the occurrence of documented lethal ventricular tachyarrhythmias (ventricular fibrillation or sustained ventricular tachycardia) or cardiac death. The secondary endpoint was admission for cardiovascular causes.
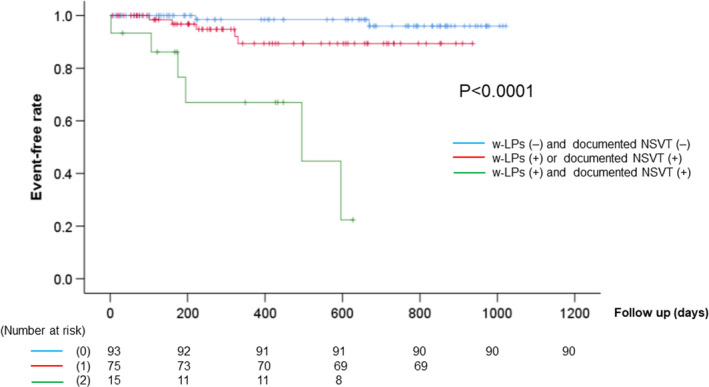
Results: Thirteen patients reached the primary endpoint during a follow-up period of 24 ± 11 months. Cox univariate regression analysis showed that existence of w-LPs (hazard ratio [HR] = 6.04, 95% confidence interval [CI]: 1.4-22.3, p = .007) and NSVT [HR = 8.72, 95% CI: 2.8-26.5: p < .001] was significantly associated with the primary endpoint. Kaplan-Meier analysis demonstrated that the combination of w-LPs and NSVT resulted in a lower event-free survival rate than did other NIEMs (p < .0001). No NIEM was useful in predicting the secondary endpoint, although the left ventricular mass index was correlated with the secondary endpoint.
Conclusion: The combination of w-LPs and NSVT was a significant risk factor for lethal ventricular tachyarrhythmias and cardiac death in CKD-SHD patients.
Keywords: ambulatory electrocardiography; chronic kidney disease; late potentials; nonsustained ventricular tachycardia; sudden cardiac death; ventricular tachycardia.
© 2021 The Authors. Annals of Noninvasive Electrocardiology published by Wiley Periodicals LLC.
Conflict of interest statement
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
Figures
Similar articles
-
Combined evaluation of ambulatory-based late potentials and nonsustained ventricular tachycardia to predict arrhythmic events in patients with previous myocardial infarction: A Japanese noninvasive electrocardiographic risk stratification of sudden cardiac death (JANIES) substudy.Ann Noninvasive Electrocardiol. 2021 Jan;26(1):e12803. doi: 10.1111/anec.12803. Epub 2020 Sep 24. Ann Noninvasive Electrocardiol. 2021. PMID: 32969113 Free PMC article.
-
Risk stratification for cardiac mortality using electrocardiographic markers based on 24-hour Holter recordings: the JANIES-SHD study.J Cardiol. 2020 Feb;75(2):155-163. doi: 10.1016/j.jjcc.2019.07.012. Epub 2019 Aug 30. J Cardiol. 2020. PMID: 31474497
-
Risk stratification for serious arrhythmic events using nonsustained ventricular tachycardia and heart rate turbulence detected by 24-hour holter electrocardiograms in patients with left ventricular dysfunction.Ann Noninvasive Electrocardiol. 2012 Jul;17(3):260-7. doi: 10.1111/j.1542-474X.2012.00522.x. Ann Noninvasive Electrocardiol. 2012. PMID: 22816545 Free PMC article.
-
Electrocardiographic predictors in the ESVEM trial: unsustained ventricular tachycardia, heart period variability, and the signal-averaged electrocardiogram.Prog Cardiovasc Dis. 1996 May-Jun;38(6):463-88. doi: 10.1016/s0033-0620(96)80011-9. Prog Cardiovasc Dis. 1996. PMID: 8638028 Review.
-
Application of noninvasive and invasive tests for risk assessment in patients with ventricular arrhythmias.Cardiol Clin. 2000 May;18(2):243-63, vii. doi: 10.1016/s0733-8651(05)70140-5. Cardiol Clin. 2000. PMID: 10849872 Review.
Cited by
-
Diurnal Variation in and Optimal Time to Measure Holter-Based Late Potentials to Predict Lethal Arrhythmia after Myocardial Infarction.Medicina (Kaunas). 2023 Aug 13;59(8):1460. doi: 10.3390/medicina59081460. Medicina (Kaunas). 2023. PMID: 37629750 Free PMC article.
-
2025 Japanese Heart Rhythm Society / Japanese Circulation Society Consensus Statement on the Appropriate Use of Ambulatory and Wearable Electrocardiographs.J Arrhythm. 2025 May 23;41(3):e70059. doi: 10.1002/joa3.70059. eCollection 2025 Jun. J Arrhythm. 2025. PMID: 40416951 Free PMC article.
-
Noninvasive Ambulatory Electrocardiographic Markers from Patients with COVID-19 Pneumonia: A Report of Three Cases.Medicina (Kaunas). 2024 Apr 19;60(4):655. doi: 10.3390/medicina60040655. Medicina (Kaunas). 2024. PMID: 38674301 Free PMC article.
References
-
- Abe, A. , Kobayashi, K. , Yuzawa, H. , Sato, H. , Fukunaga, S. , Fujino, T. , Okano, Y. , Yamazaki, J. , Miwa, Y. , Yoshino, H. , & Ikeda, T. (2012). Comparison of late potentials for 24 hours between Brugada syndrome and arrhythmogenic right ventricular cardiomyopathy using a novel signal‐averaging system based on Holter ECG. Circulation: Arrhythmia and Electrophysiology, 5, 789–795. 10.1161/CIRCEP.111.969865 - DOI - PubMed
-
- Bauer, A. , Malik, M. , Schmidt, G. , Barthel, P. , Bonnemeier, H. , Cygankiewicz, I. , Guzik, P. , Lombardi, F. , Müller, A. , Oto, A. , Schneider, R. , Watanabe, M. , Wichterle, D. , & Zareba, W. (2008). Heart rate turbulence: Standards of measurement, physiological interpretation, and clinical use: International Society for Holter and Noninvasive Electrophysiology Consensus. Journal of the American College of Cardiology, 52, 1353–1365. 10.1016/j.jacc.2008.07.041 - DOI - PubMed
-
- Daimon, M. , Watanabe, H. , Abe, Y. , Hirata, K. , Hozumi, T. , Ishii, K. , Ito, H. , Iwakura, K. , Izumi, C. , Matsuzaki, M. , Minagoe, S. , Abe, H. , Murata, K. , Nakatani, S. , Negishi, K. , Yoshida, K. , Tanabe, K. , Tanaka, N. , Tokai, K. , … The JAMP Study Investigators . (2008). Normal values of echocardiographic parameters in relation to age in a healthy Japanese population: The JAMP study. Circulation Journal, 72, 1859–1866. 10.1253/circj.cj-08-0171 - DOI - PubMed
-
- Dubin, R. F. , Deo, R. , Bansal, N. , Anderson, A. H. , Yang, P. , Go, A. S. , Keane, M. , Townsend, R. , Porter, A. , Budoff, M. , Malik, S. , He, J. , Rahman, M. , Wright, J. , Cappola, T. , Kallem, R. , Roy, J. , Sha, D. , & Shlipak, M. G. (2017). Associations of conventional echocardiographic measures with incident heart failure and mortality: The chronic renal insufficiency cohort. Clinical Journal of the American Society of Nephrology, 12, 60–68. 10.2215/CJN.02700316 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
