

Persistent Tennis Elbow Symptoms Have Little Prognostic Value: A Systematic Review and Meta-analysis
- PMID: 34874323
- PMCID: PMC8923574
- DOI: 10.1097/CORR.0000000000002058
Persistent Tennis Elbow Symptoms Have Little Prognostic Value: A Systematic Review and Meta-analysis
Abstract
Background: Tennis elbow is a common painful enthesopathy of the lateral elbow that limits upper limb function and frequently results in lost time at work. Surgeons often recommend surgery if symptoms persist despite nonsurgical management, but operations for tennis elbow are inconsistent in their efficacy, and what we know about those operations often derives from observational studies that assume the condition does not continue to improve over time. This assumption is largely untested, and it may not be true; meta-analyzing results from the control arms of tennis elbow studies can help us to evaluate this premise, but to our knowledge, this has not been done.
Questions/purposes: The aims of this systematic review were to describe the course of (1) global improvement, (2) pain, and (3) disability in participants who received no active treatment (placebo or no treatment) in published randomized controlled trials (RCTs) on tennis elbow. We also assessed (4) whether the duration of symptoms or placebo effect is associated with differences in symptom trajectories.
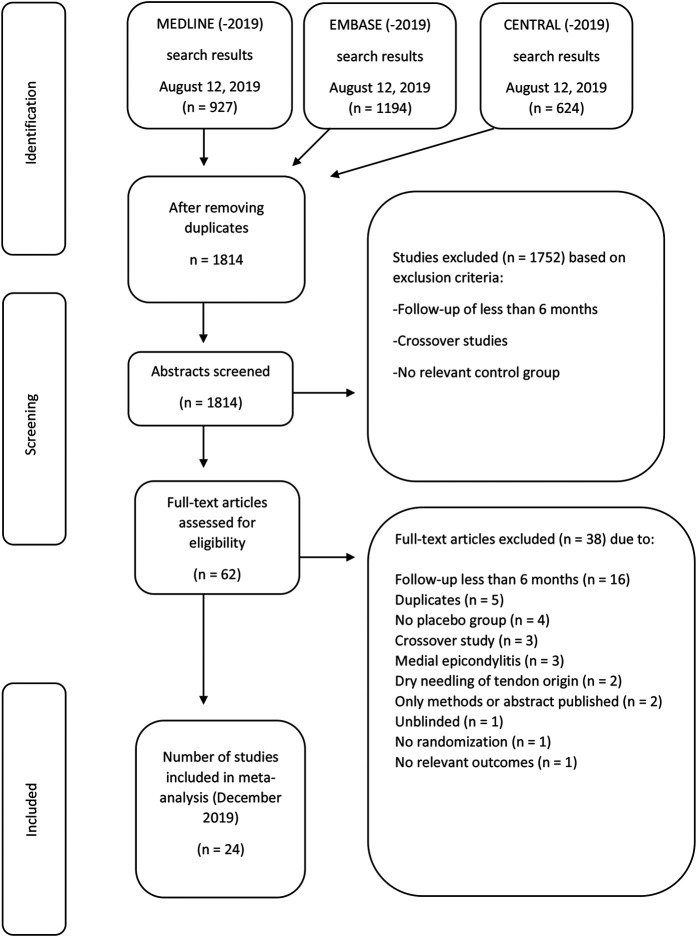
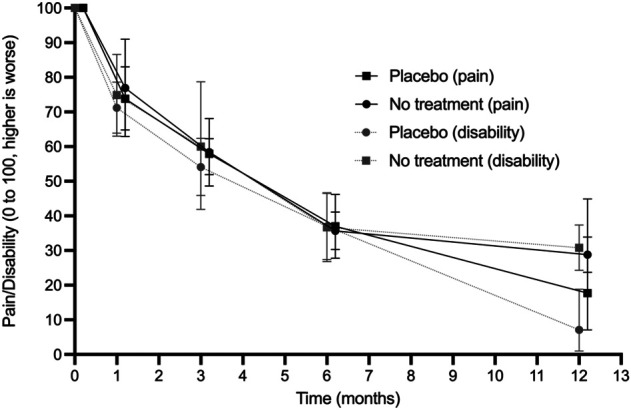
Methods: We searched MEDLINE, Embase, and CENTRAL from database inception to August 12, 2019, for trials including participants with tennis elbow and a placebo or a no-treatment arm and a minimum follow-up duration of 6 months. There were no language restrictions or exclusion criteria. We extracted global improvement, pain, and disability outcomes. We used the Cochrane Risk of Bias tool to assess the risk of bias of included trials. To estimate the typical course of tennis elbow without active treatment, we pooled global improvement (the proportion of participants who reported feeling much better or completely recovered), mean pain, and mean disability using baseline, 1-month, 3-month, 6-month, and 12-month follow-up data. We transformed pain and disability data from the original papers so that at each timepoint the relevant outcome was expressed as change relative to baseline to account for different baseline values. We used meta-regression to assess whether the placebo effect or duration of symptoms before enrollment was associated with differences in symptom trajectories. We included 24 trials with 1085 participants who received no active treatment.
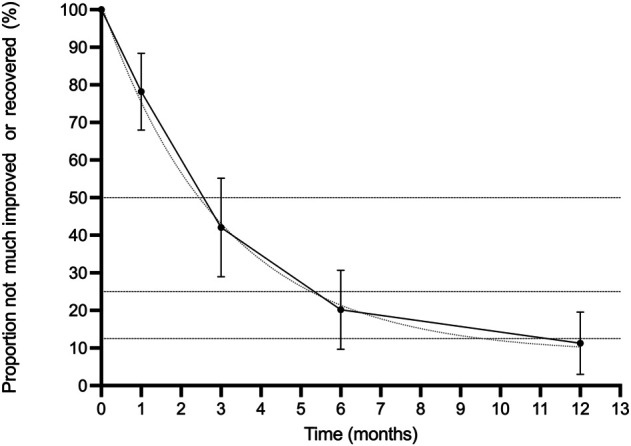
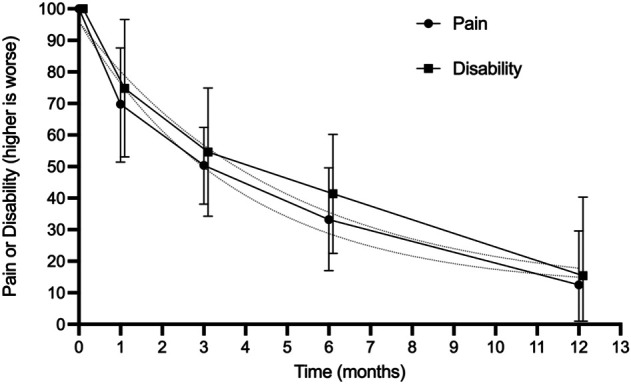
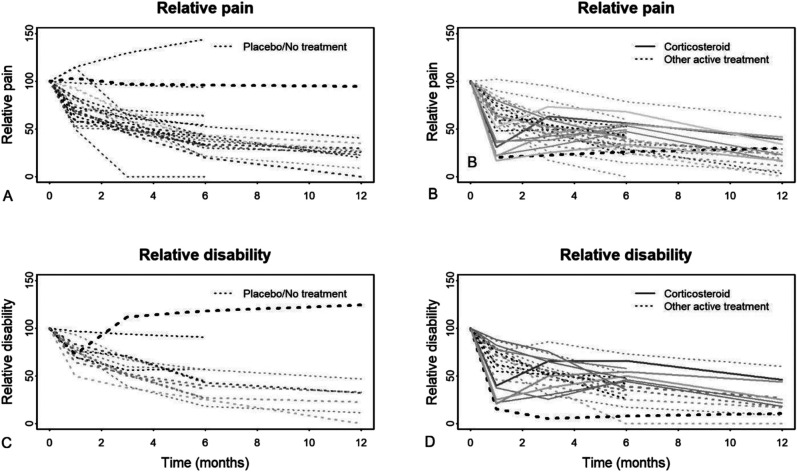
Results: The number of patients who were not improved decreased exponentially over time. The half-life of global improvement was between 2.5 and 3 months (that is, every 2.5 to 3 months, 50% of the remaining symptomatic patients reported complete recovery or greatly improved symptoms). At 1 year, 89% (189 of 213; 95% CI 80% to 97%) of patients experienced global improvement. The mean pain and disability followed a similar pattern, halving every 3 to 4 months. Eighty-eight percent of pain (95% CI 70% to 100%) and 85% of disability (95% CI 60% to 100%) had resolved by 1 year. The mean duration of symptoms before trial enrollment was not associated with differences in symptom trajectories. The trajectories of the no-treatment and placebo arms were similar, indicating that the placebo effect of the studied active treatments likely is negligible.
Conclusion: Based on the placebo or no-treatment control arms of randomized trials, about 90% of people with untreated tennis elbow achieve symptom resolution at 1 year. The probability of resolution appears to remain constant throughout the first year of follow-up and does not depend on previous symptom duration, undermining the rationale that surgery is appropriate if symptoms persist beyond a certain point of time. We recommend that clinicians inform people who are frustrated with persisting symptoms that this is not a cause for apprehension, given that spontaneous improvement is about as likely during the subsequent few months as it was early after the symptoms first appeared. Because of the high likelihood of spontaneous recovery, any active intervention needs to be justified by high levels of early efficacy and little or no risk to outperform watchful waiting.
Level of evidence: Level I, therapeutic study.
Copyright © 2021 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
Editor's Spotlight/Take 5: Persistent Tennis Elbow Symptoms Have Little Prognostic Value: A Systematic Review and Meta-analysis.Clin Orthop Relat Res. 2022 Apr 1;480(4):642-646. doi: 10.1097/CORR.0000000000002149. Clin Orthop Relat Res. 2022. PMID: 35171124 Free PMC article. No abstract available.
-
Letter to the Editor: Persistent Tennis Elbow Symptoms Have Little Prognostic Value: A Systematic Review and Meta-analysis.Clin Orthop Relat Res. 2022 Aug 1;480(8):1616-1617. doi: 10.1097/CORR.0000000000002254. Epub 2022 May 24. Clin Orthop Relat Res. 2022. PMID: 35608414 Free PMC article. No abstract available.
References
-
- Åkermark C, Crone H, Elsasser U, Forsskahl B. Glycosaminoglycan polysulfate injections in lateral humeral epicondylalgia: a placebo-controlled double-blind trial. Int J Sports Med. 1995;16:196-200. - PubMed
-
- Artus M, van der Windt DA, Jordan KP, Hay EM. Low back pain symptoms show a similar pattern of improvement following a wide range of primary care treatments: a systematic review of randomized clinical trials. Rheumatology (Oxford) . 2010;49:2346‐2356. - PubMed
-
- Barnett AG, van der Pols JC, Dobson AJ. Regression to the mean: what it is and how to deal with it. Int J Epidemiol . 2005;34:215-220. - PubMed
-
- Bisset L, Smidt N, Van Der Windt D, et al. Conservative treatments for tennis elbow do subgroups of patients respond differently? Rheumatology (Oxford) . 2007;46:1601-1605. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
