

Pneumatocele formation following COVID-19 pneumonia. Is there a role for surgical intervention?
- PMID: 34874785
- PMCID: PMC9174975
- DOI: 10.1177/02184923211059866
Pneumatocele formation following COVID-19 pneumonia. Is there a role for surgical intervention?
Abstract
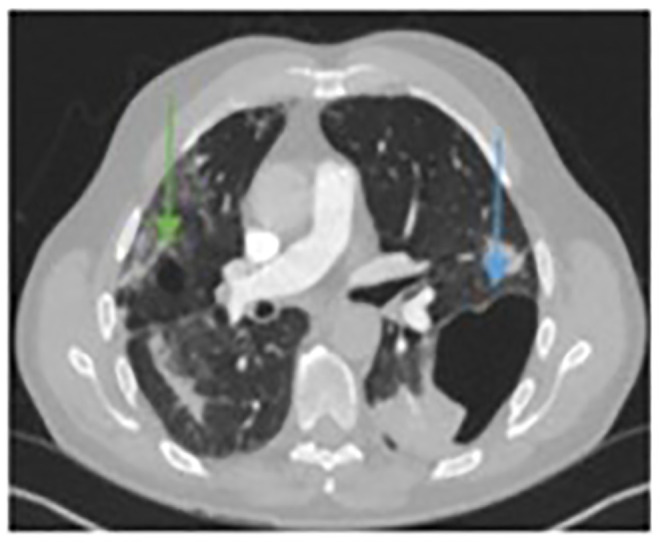
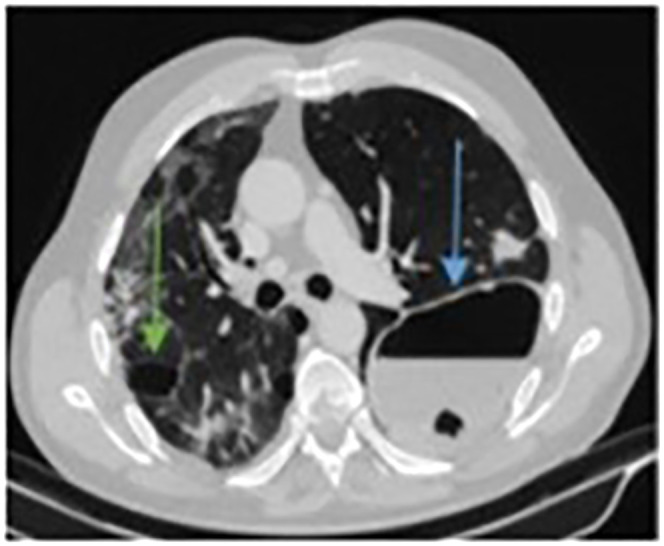
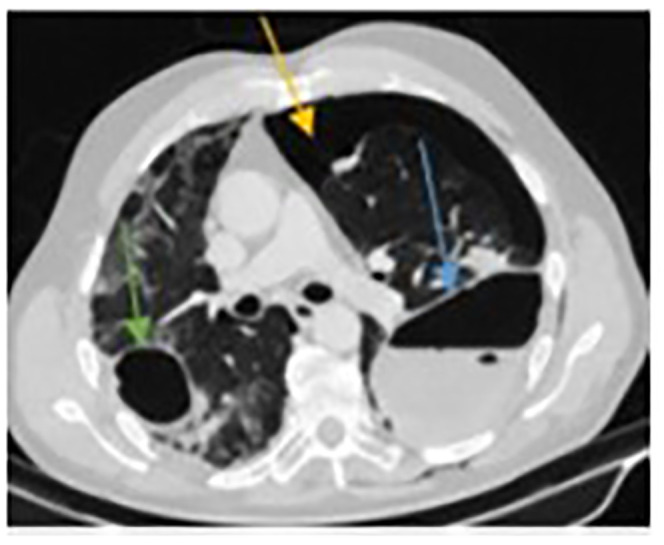
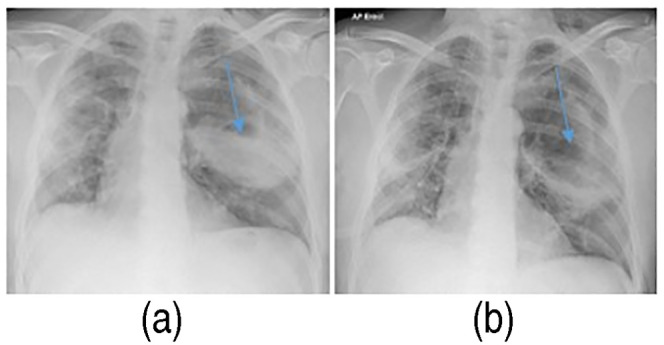
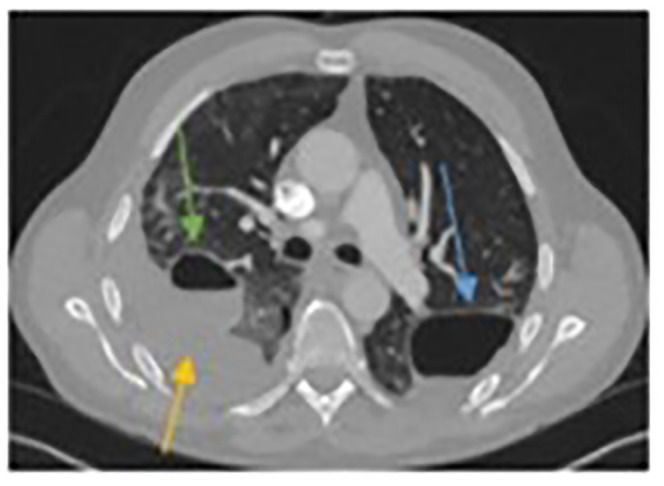
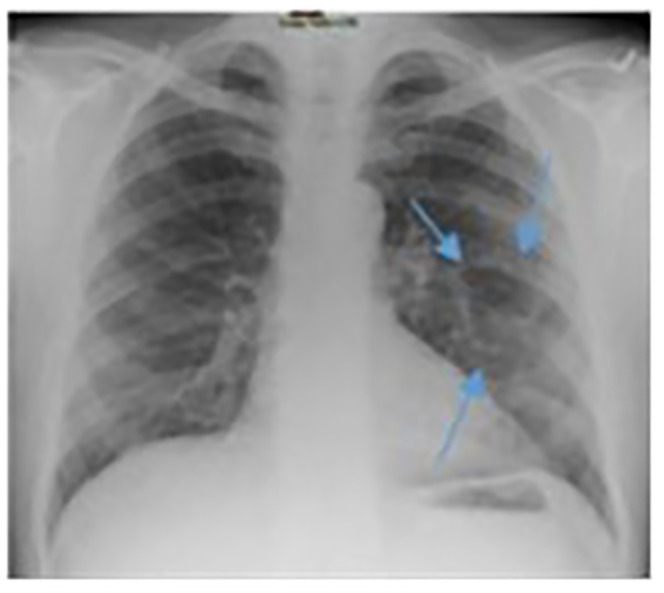
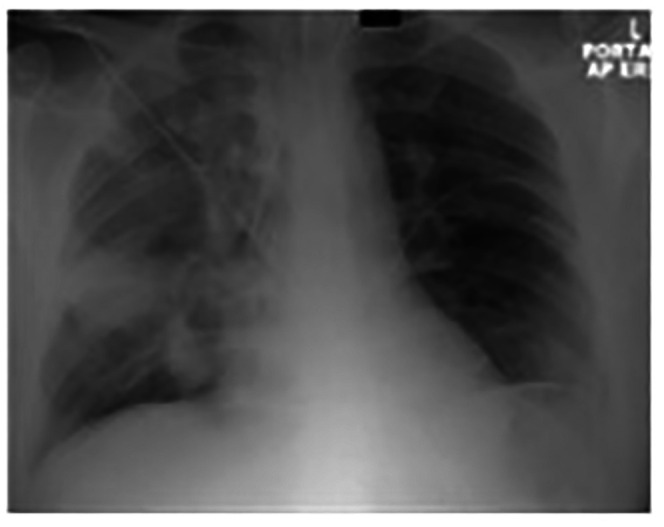
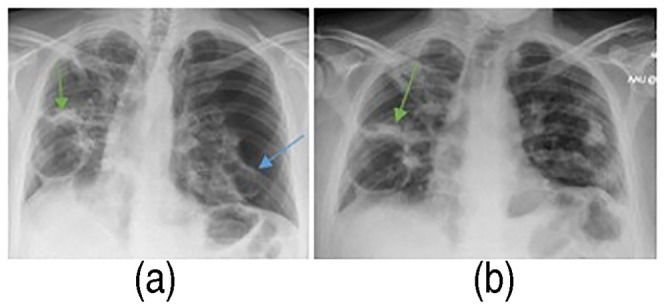
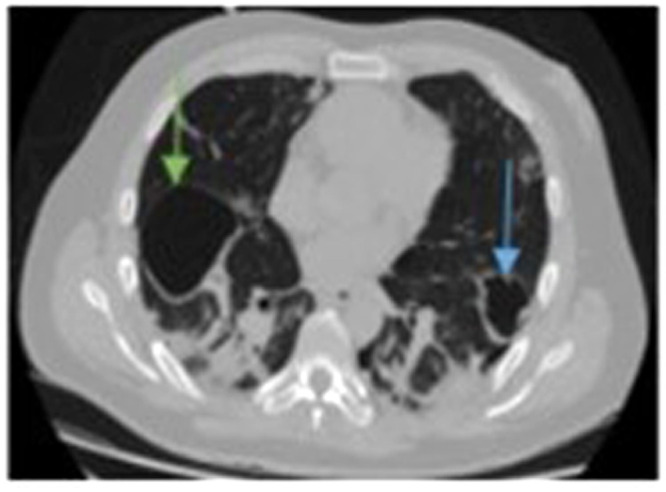
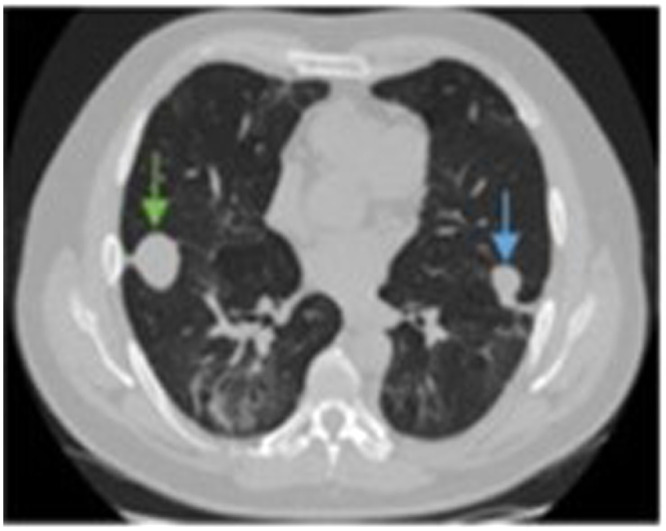
COVID-19 mainly causes a lower respiratory tract illness, meaning there has been great interest in the chest and lung radiological findings seen during the course of the disease. Most of this interest has centred around the computed tomographic findings. Most commonly, computed tomographic images report ground-glass opacities but a less common finding, and potential complication associated with COVID-19, is pneumatocele formation. In this case series, we describe the presentation and management of three patients with large pneumatoceles that developed during the recovery phase of COVID-19. A conservative approach is most recommended, with surgical intervention reserved for complicated cases that cause cardiorespiratory compromise.
Keywords: COVID-19; Pneumatocele; pneumothorax; thorax.
Conflict of interest statement
Figures



References
-
- Wu J, Feng LC, Xian XY, et al. Novel coronavirus pneumonia (COVID-19) CT distribution and sign features. Zhonghua Jie He He Hu Xi Za Zhi 2020; 43: 321–326. - PubMed
-
- Serebrisky D, Atlas AB, Boyer D. Pneumatocele. Medscape. Accessed 18/04/2021. <https://emedicine.medscape.com/article/1003289-overview>. 2016.
LinkOut - more resources
Full Text Sources
