

Alveolar epithelial glycocalyx degradation mediates surfactant dysfunction and contributes to acute respiratory distress syndrome
- PMID: 34874923
- PMCID: PMC8855818
- DOI: 10.1172/jci.insight.154573
Alveolar epithelial glycocalyx degradation mediates surfactant dysfunction and contributes to acute respiratory distress syndrome
Abstract
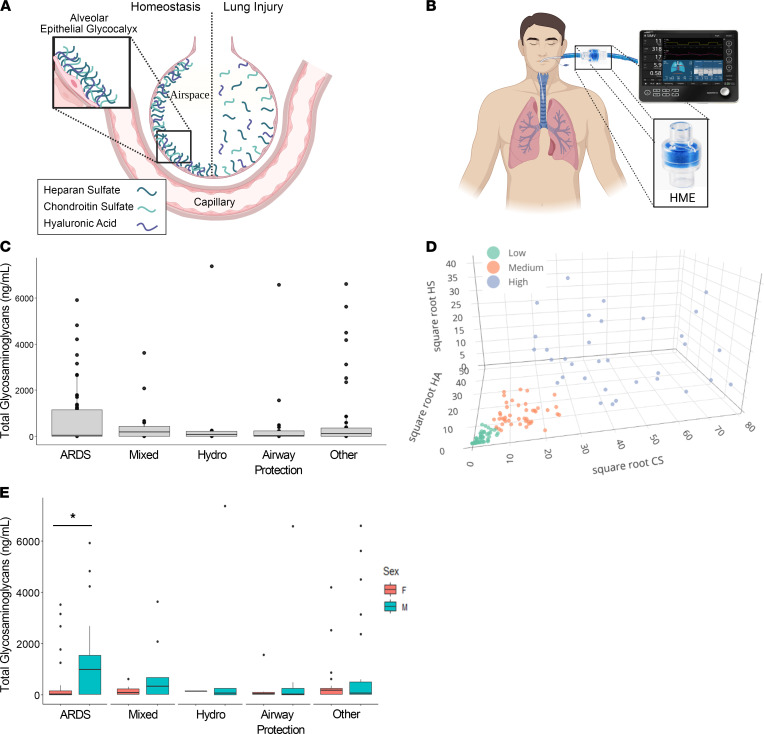
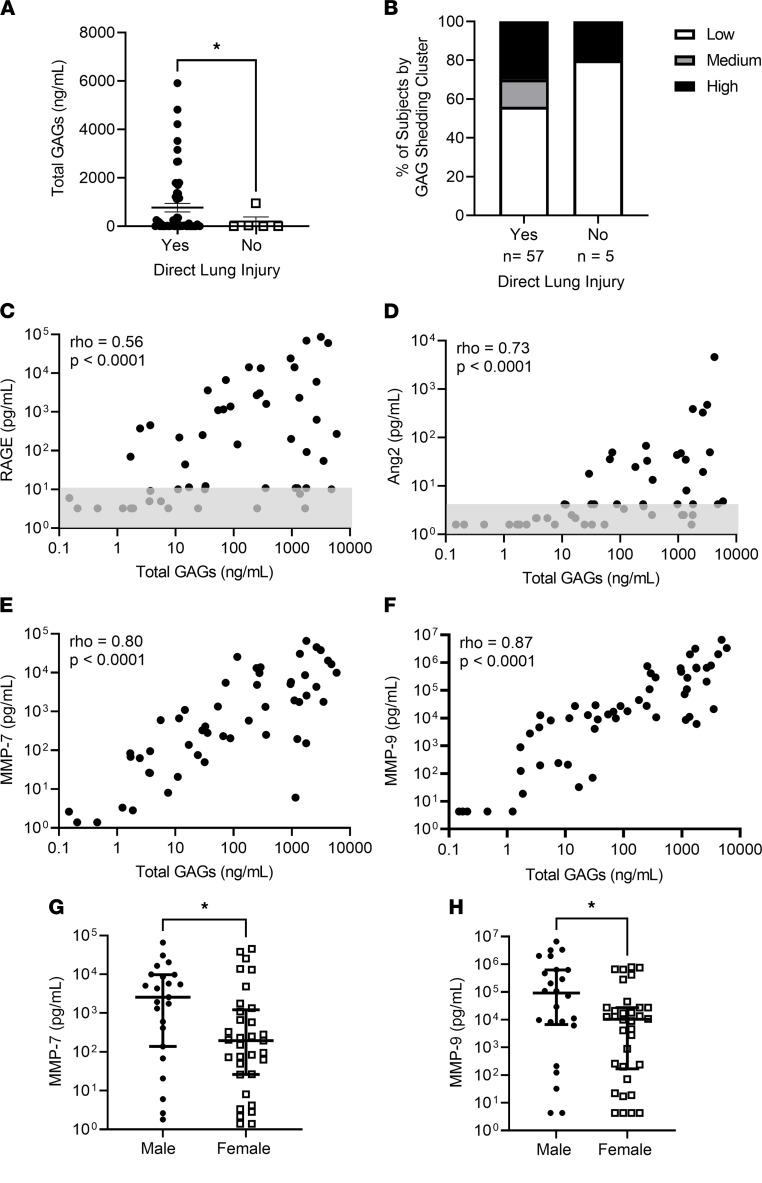
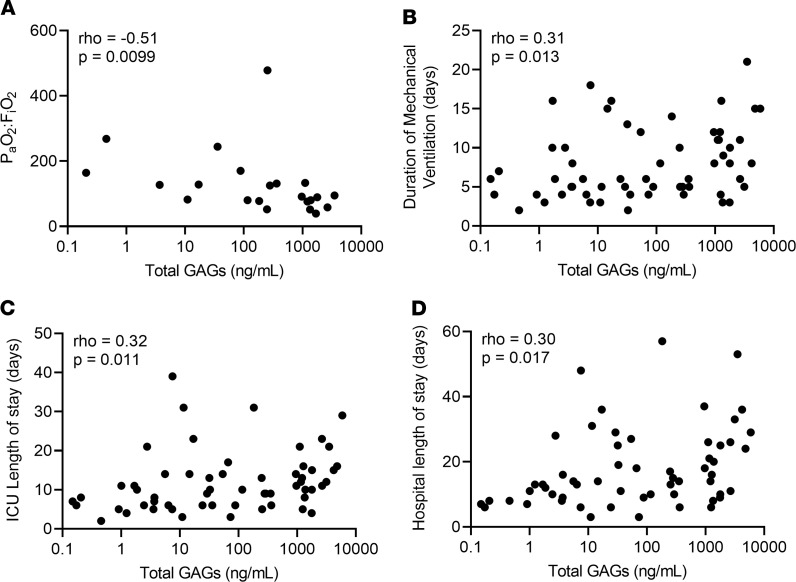
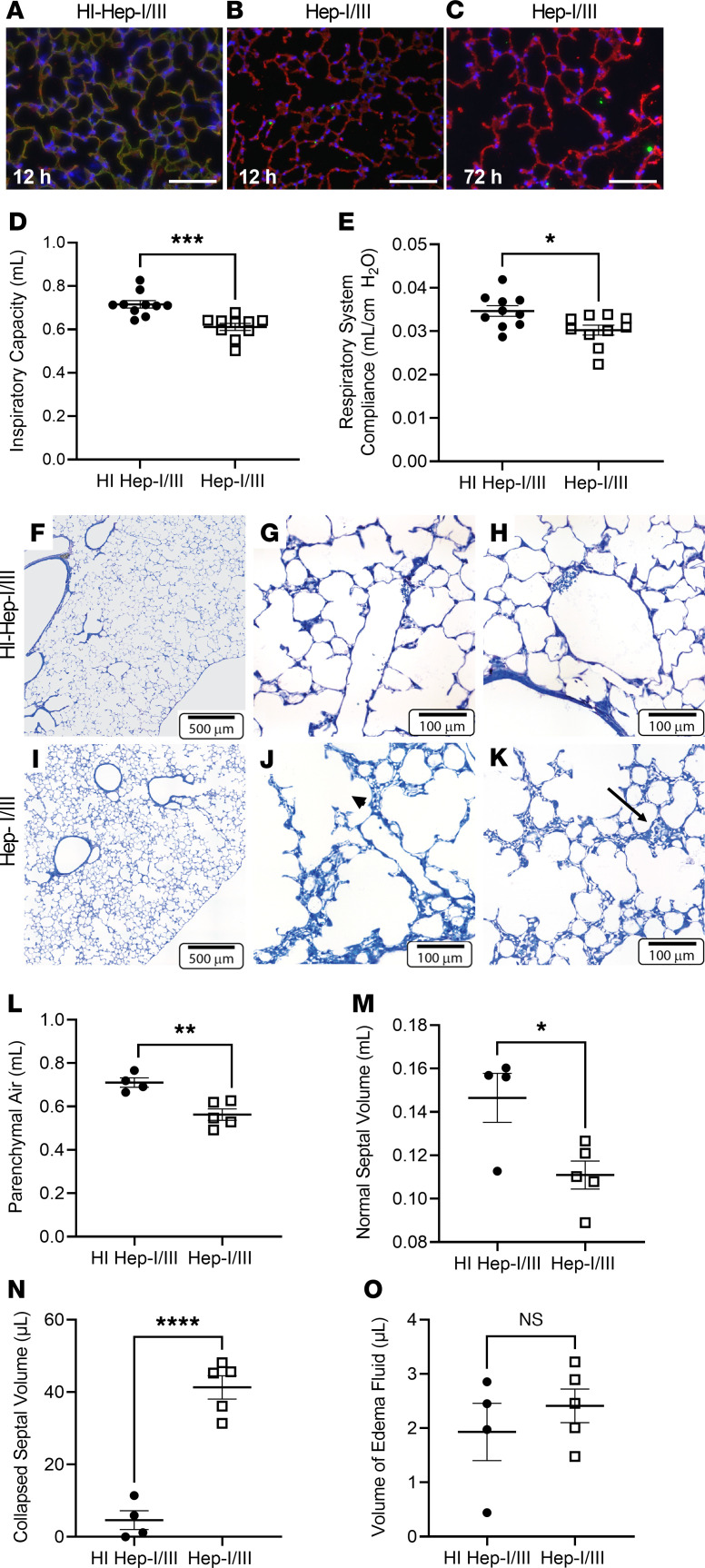
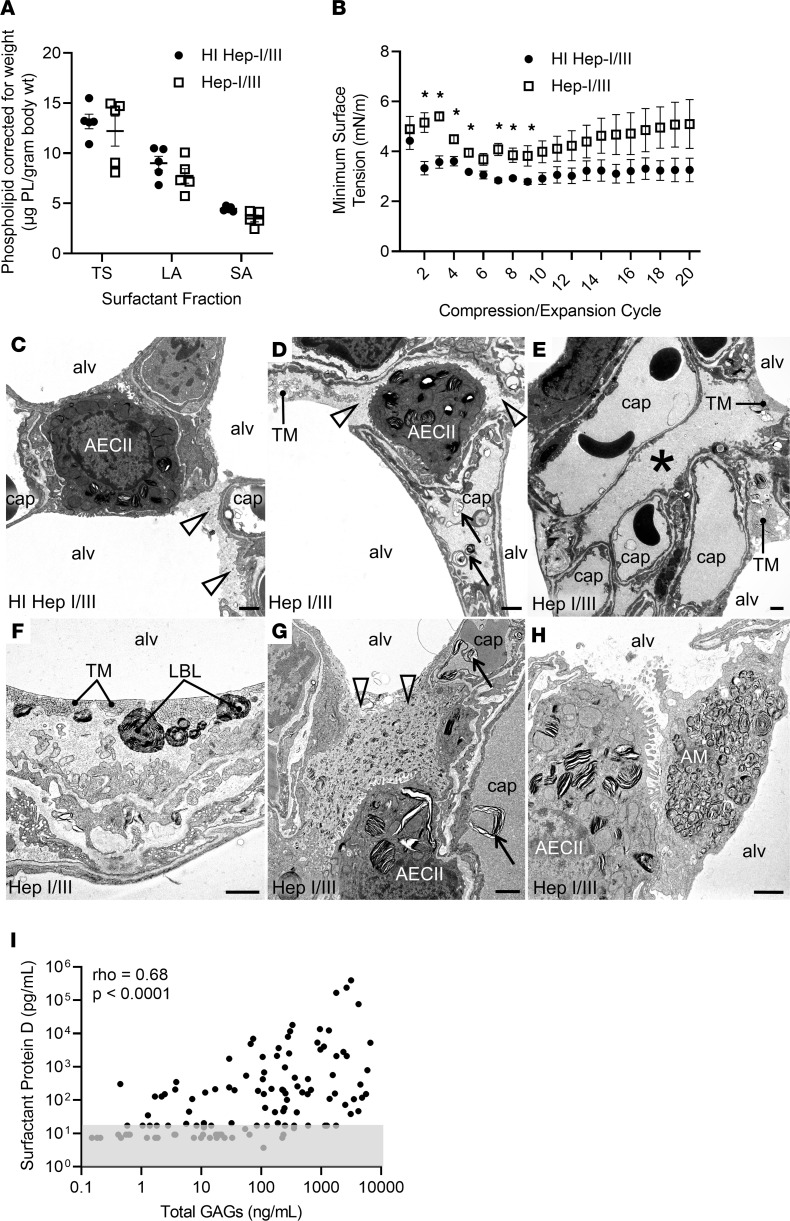
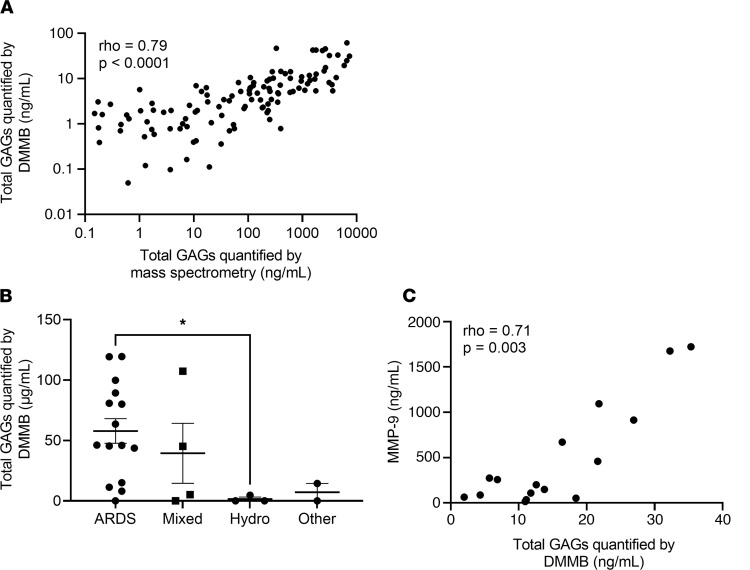
Acute respiratory distress syndrome (ARDS) is a common cause of respiratory failure yet has few pharmacologic therapies, reflecting the mechanistic heterogeneity of lung injury. We hypothesized that damage to the alveolar epithelial glycocalyx, a layer of glycosaminoglycans interposed between the epithelium and surfactant, contributes to lung injury in patients with ARDS. Using mass spectrometry of airspace fluid noninvasively collected from mechanically ventilated patients, we found that airspace glycosaminoglycan shedding (an index of glycocalyx degradation) occurred predominantly in patients with direct lung injury and was associated with duration of mechanical ventilation. Male patients had increased shedding, which correlated with airspace concentrations of matrix metalloproteinases. Selective epithelial glycocalyx degradation in mice was sufficient to induce surfactant dysfunction, a key characteristic of ARDS, leading to microatelectasis and decreased lung compliance. Rapid colorimetric quantification of airspace glycosaminoglycans was feasible and could provide point-of-care prognostic information to clinicians and/or be used for predictive enrichment in clinical trials.
Keywords: Glycobiology; Proteoglycans; Pulmonary surfactants; Pulmonology.
Conflict of interest statement
Figures
Similar articles
-
The role of the alveolar epithelial glycocalyx in acute respiratory distress syndrome.Am J Physiol Cell Physiol. 2023 Apr 1;324(4):C799-C806. doi: 10.1152/ajpcell.00555.2022. Epub 2023 Feb 27. Am J Physiol Cell Physiol. 2023. PMID: 36847444 Free PMC article. Review.
-
Alveolar epithelial glycocalyx shedding aggravates the epithelial barrier and disrupts epithelial tight junctions in acute respiratory distress syndrome.Biomed Pharmacother. 2021 Jan;133:111026. doi: 10.1016/j.biopha.2020.111026. Epub 2020 Nov 24. Biomed Pharmacother. 2021. PMID: 33378942 Free PMC article.
-
Epithelial Heparan Sulfate Contributes to Alveolar Barrier Function and Is Shed during Lung Injury.Am J Respir Cell Mol Biol. 2018 Sep;59(3):363-374. doi: 10.1165/rcmb.2017-0428OC. Am J Respir Cell Mol Biol. 2018. PMID: 29584451 Free PMC article.
-
Matrix metalloproteinases mediate influenza A-associated shedding of the alveolar epithelial glycocalyx.PLoS One. 2024 Sep 23;19(9):e0308648. doi: 10.1371/journal.pone.0308648. eCollection 2024. PLoS One. 2024. PMID: 39312544 Free PMC article.
-
Hyperpolarized gas diffusion MRI for the study of atelectasis and acute respiratory distress syndrome.NMR Biomed. 2014 Dec;27(12):1468-78. doi: 10.1002/nbm.3136. Epub 2014 Jun 11. NMR Biomed. 2014. PMID: 24920074 Free PMC article. Review.
Cited by
-
Biophysical properties of alveolar surfactant in drever dogs with hunting associated pulmonary edema.Acta Vet Scand. 2024 May 31;66(1):24. doi: 10.1186/s13028-024-00745-x. Acta Vet Scand. 2024. PMID: 38822358 Free PMC article.
-
Roles of airway and intestinal epithelia in responding to pathogens and maintaining tissue homeostasis.Front Cell Infect Microbiol. 2024 Apr 26;14:1346087. doi: 10.3389/fcimb.2024.1346087. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 38736751 Free PMC article. Review.
-
Alveolar glycocalyces during health and critical illness.Proteoglycan Res. 2025 Jan-Mar;3(1):e70022. doi: 10.1002/pgr2.70022. Epub 2025 Mar 5. Proteoglycan Res. 2025. PMID: 40242042
-
Pneumomediastinum and pneumothorax in acute respiratory distress syndrome (ARDS) patients: a narrative review.Mediastinum. 2023 Dec 12;8:3. doi: 10.21037/med-23-39. eCollection 2024. Mediastinum. 2023. PMID: 38322185 Free PMC article. Review.
-
Antenatal Endotoxin Induces Dysanapsis in Experimental Bronchopulmonary Dysplasia.Am J Respir Cell Mol Biol. 2024 Apr;70(4):283-294. doi: 10.1165/rcmb.2023-0157OC. Am J Respir Cell Mol Biol. 2024. PMID: 38207120 Free PMC article.
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
- TL1 TR002533/TR/NCATS NIH HHS/United States
- R01 HL149422/HL/NHLBI NIH HHS/United States
- T32 GM007635/GM/NIGMS NIH HHS/United States
- T32 HL007085/HL/NHLBI NIH HHS/United States
- F32 HL162230/HL/NHLBI NIH HHS/United States
- T32 HL072738/HL/NHLBI NIH HHS/United States
- R01 GM125095/GM/NIGMS NIH HHS/United States
- R01 HL135849/HL/NHLBI NIH HHS/United States
- K08 HL136888/HL/NHLBI NIH HHS/United States
- K24 HL103836/HL/NHLBI NIH HHS/United States
- K01 HL157755/HL/NHLBI NIH HHS/United States
- P01 HL152961/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
