

Prognostic scores and early management of septic patients in the emergency department of a secondary hospital: results of a retrospective study
- PMID: 34876007
- PMCID: PMC8650550
- DOI: 10.1186/s12873-021-00547-8
Prognostic scores and early management of septic patients in the emergency department of a secondary hospital: results of a retrospective study
Abstract
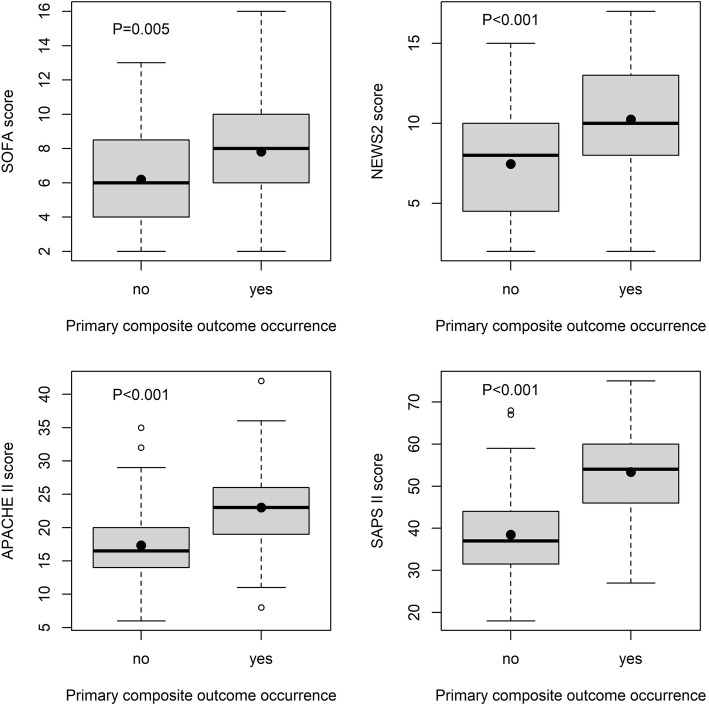
Background: Sequential Organ Failure Assessment (SOFA) and other illness prognostic scores predict adverse outcomes in critical patients. Their validation as a decision-making tool in the emergency department (ED) of secondary hospitals is not well established. The aim of this study was to compare SOFA, NEWS2, APACHE II, and SAPS II scores as predictors of adverse outcomes and decision-making tool in ED.
Methods: Data of 121 patients (age 73 ± 10 years, 58% males, Charlson Comorbidity Index 5.7 ± 2.1) with a confirmed sepsis were included in a retrospective study between January 2017 and February 2020. Scores were computed within the first 24 h after admission. Primary outcome was the occurrence of either in-hospital death or mechanical ventilation within 7 days. Secondary outcome was 30-day all-cause mortality.
Results: Patients older than 64 years (elderly) represent 82% of sample. Primary and secondary outcomes occurred in 40 and 44%, respectively. Median 30-day survival time of dead patients was 4 days (interquartile range 1-11). The best predictive score based on the area under the receiver operating curve (AUROC) was SAPS II (0.823, 95% confidence interval, CI, 0.744-0.902), followed by APACHE II (0.762, 95% CI 0.673-0.850), NEWS2 (0.708, 95% CI 0.616-0.800), and SOFA (0.650, 95% CI 0.548-0.751). SAPS II cut-off of 49 showed the lowest false-positive rate (12, 95% CI 5-20) and the highest positive predictive value (80, 95% CI 68-92), whereas NEWS2 cut-off of 7 showed the lowest false-negative rate (10, 95% CI 2-19) and the highest negative predictive value (86, 95% CI 74-97). By combining NEWS2 and SAPS II cut-offs, we accurately classified 64% of patients. In survival analysis, SAPS II cut-off showed the highest difference in 30-day mortality (Hazards Ratio, HR, 5.24, 95% CI 2.99-9.21, P < 0.001). Best independent negative predictors of 30-day mortality were body temperature, mean arterial pressure, arterial oxygen saturation, and hematocrit levels. Positive predictors were male sex, heart rate and serum sodium concentration.
Conclusions: SAPS II is a good prognostic tool for discriminating high-risk patient suitable for sub-intensive/intensive care units, whereas NEWS2 for discriminating low-risk patients for low-intensive units. Our results should be limited to cohorts with a high prevalence of elderly or comorbidities.
Keywords: APACHE II; NEWS2; ROC curve; SAPS II; SOFA; Survival analysis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A, Rubenfeld G, Kahn JM, Shankar-Hari M, Singer M, Deutschman CS, Escobar GJ, Angus DC. Assessment of clinical criteria for Sepsis: for the third international consensus definitions for Sepsis and septic shock (Sepsis-3) JAMA. 2016;315(8):762–774. doi: 10.1001/jama.2016.0288. - DOI - PMC - PubMed
-
- Freund Y, Lemachatti N, Krastinova E, Van Laer M, Claessens Y-E, Avondo A, et al. Prognostic accuracy of Sepsis-3 criteria for in-hospital mortality among patients with suspected infection presenting to the emergency department. JAMA. 2017;317(3):301–308. doi: 10.1001/jama.2016.20329. - DOI - PubMed
-
- Askim Å, Moser F, Gustad LT, Stene H, Gundersen M, Åsvold BO, Dale J, Bjørnsen LP, Damås JK, Solligård E. Poor performance of quick-SOFA (qSOFA) score in predicting severe sepsis and mortality - a prospective study of patients admitted with infection to the emergency department. Scand J Trauma Resusc Emerg Med. 2017;25(1):56. doi: 10.1186/s13049-017-0399-4. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
