

Hypercortisolism in patients with cholestasis is associated with disease severity
- PMID: 34876016
- PMCID: PMC8650422
- DOI: 10.1186/s12876-021-02045-4
Hypercortisolism in patients with cholestasis is associated with disease severity
Abstract
Background: Cholestasis might lead to an impairment of adrenal function as suggested by in vitro and in vivo data as well as by clinical findings. Bile acid and adrenal steroid metabolism not only share the receptors farnesoid X receptor (FXR) and the G protein-coupled bile acid receptor 1 (TGR5), but supraphysiological bile acid levels were found to stimulate steroidogenesis independent of FXR and TGR5. Our previous experimental findings revealed that mice fed bile acids or subjected to common bile duct ligation develop hypercortisolemia. We thus aimed to assess adrenal gland function in patients with cholestasis.
Methods: Adrenal gland function was assessed in 36 patients with cholestasis and in 32 patients without cholestasis by measuring total serum cortisol, adrenocorticotropic hormone (ACTH), as well as the increase of cortisol 20 and 30 min after administration of 1 µg of ACTH. Bile acid levels and bile acid pool composition were determined by high-resolution mass spectrometry.
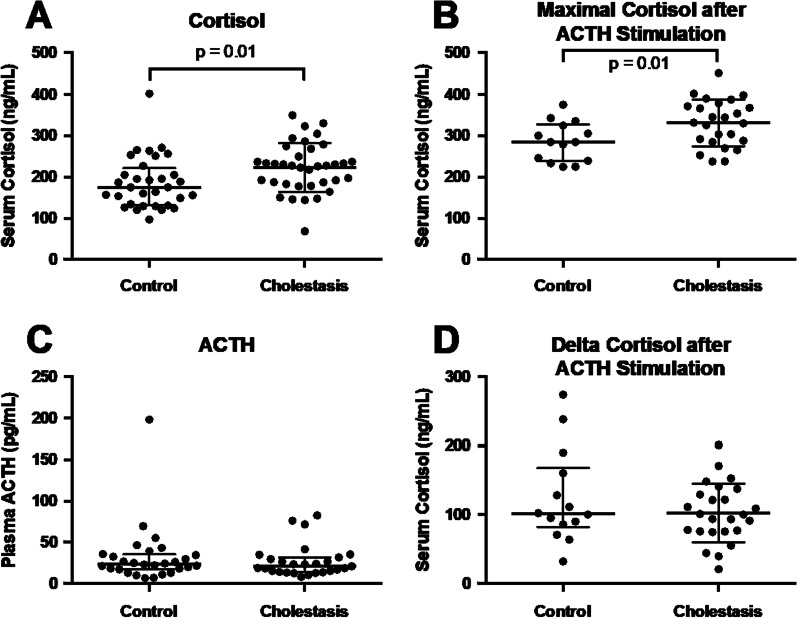
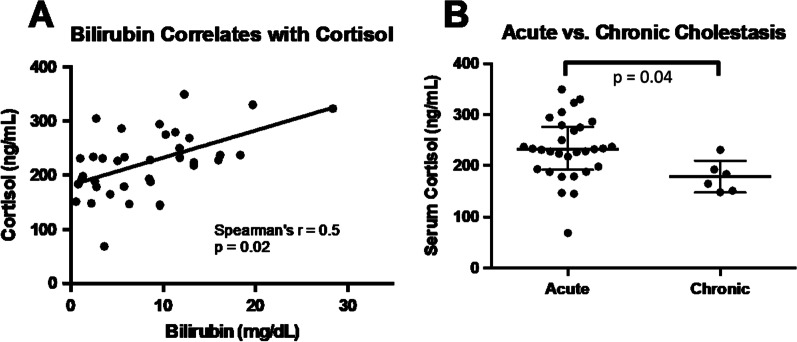
Results: Patients with cholestasis per definition had markedly elevated levels of alkaline phosphatase (AP), bilirubin and serum bile acids. Baseline cortisol and maximum cortisol after ACTH stimulation were significantly higher in patients with cholestasis compared to controls. Increase of cortisol after ACTH stimulation and ACTH did not differ. In the cholestasis group, baseline cortisol correlated with bilirubin but not with AP, total serum bile acids and levels of conjugated and unconjugated bile acid species. Patients with duration of cholestasis < 6 months (n = 30) had significantly higher baseline cortisol levels than those with long standing cholestasis (> 6 months), together with higher bilirubin levels.
Conclusions: We find no evidence of adrenal insufficiency in non-cirrhotic patients with cholestasis. In contrast, patients with cholestasis show hypercortisolism associated with disease severity as mirrored by levels of bilirubin. Lack of ACTH increase in cholestasis suggests a direct effect of cholestasis on adrenals and not on the pituitary gland. Further studies are needed to elucidate the mechanism of cortisol elevation in patients with cholestasis and its clinical significance.
Keywords: Adrenal gland; Bile acids; Bilirubin; Cholestasis; Cortisol; Hypothalamic–pituitary–adrenal axis (HPA axis).
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
