

Helicopter emergency medical service for time critical interfacility transfers of patients with cardiovascular emergencies
- PMID: 34876188
- PMCID: PMC8650228
- DOI: 10.1186/s13049-021-00981-4
Helicopter emergency medical service for time critical interfacility transfers of patients with cardiovascular emergencies
Abstract
Background: The goal of improving quality through centralisation of specialised medical services must be balanced against potential harm caused by delayed access to emergency treatments in rural areas. This study aims to assess the duration of transfers of critically ill patients with cardiovascular emergencies from smaller hospitals to major medical centres by a helicopter emergency medical service (HEMS) in Switzerland.
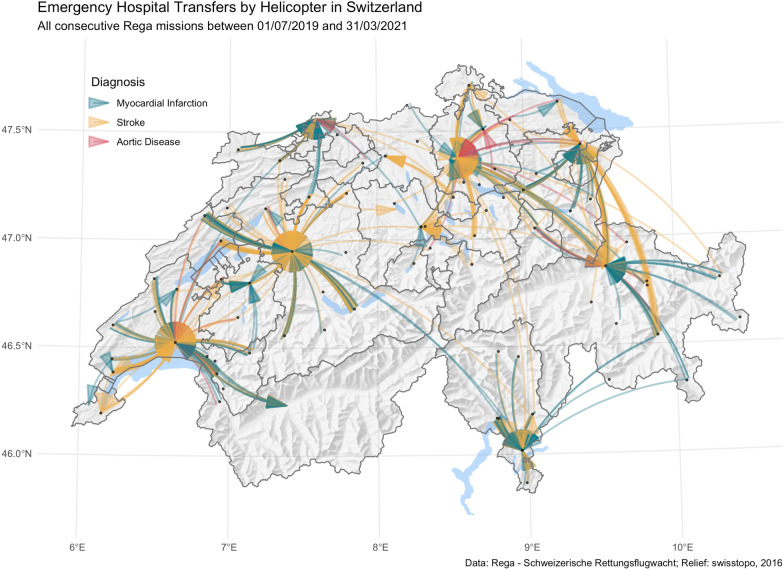
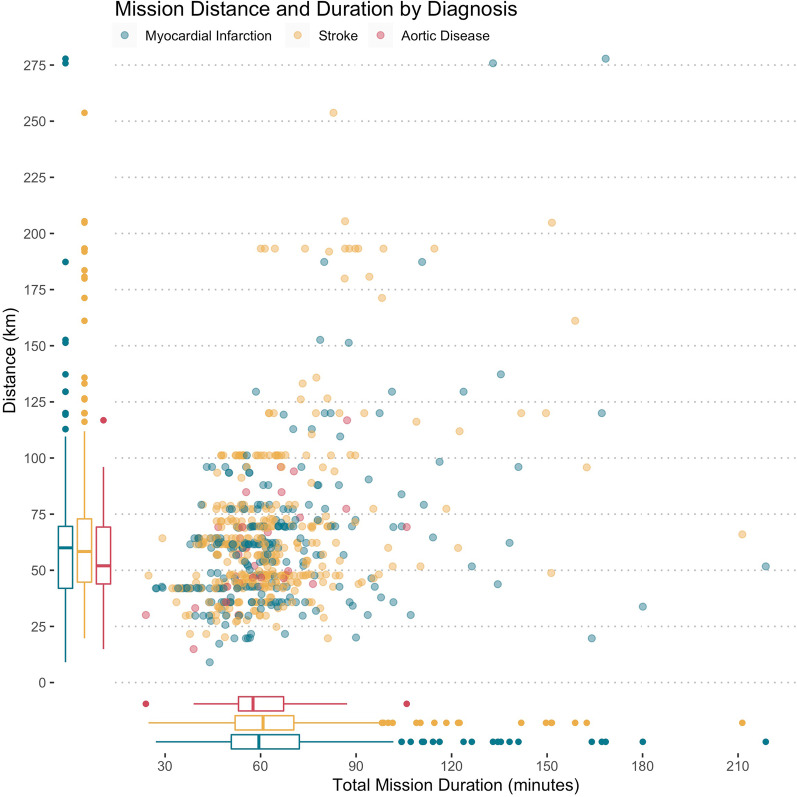
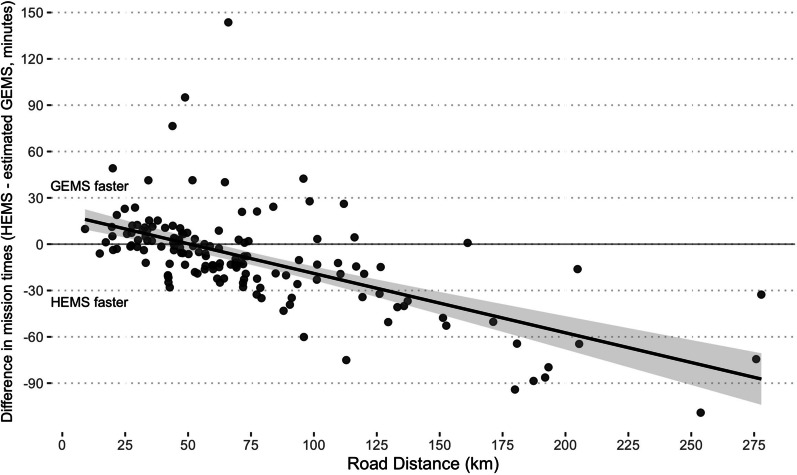
Methods: This retrospective observational cohort study includes all consecutive emergency interfacility transfers (IFTs) conducted by Switzerland's largest HEMS provider between July 3rd, 2019, and March 31st, 2021. All patients with acute myocardial infarction, non-traumatic strokes, ruptured aortic aneurysms, and other acute vascular emergencies were included. The duration and distance of each HEMS IFT were compared to calculated distances and duration of travel for the same missions using ground-based transportation (GEMS). The ground-based mission distance beyond which the total mission duration of HEMS is expected to be faster than GEMS was calculated.
Findings: A total of 645 patients were transferred for stroke (n = 364), myocardial infarction (n = 252) and other acute vascular emergencies (n = 29). The median total mission duration from emergency call to landing at the destination was 59.9 (IQR 51.5 to 70.5) minutes. The median road distance for the same missions was 60 (IQR 43 to 72) km. Regression analysis revealed that HEMS is expected to be faster if the road distance is more than 51.3 km.
Interpretation: Centralisation of specialised medical services should be accompanied by a comprehensive and specialised rescue chain. HEMS in Switzerland ensures time-sensitive IFT in medical emergencies, even in topographically challenging terrain.
Keywords: Cardiovascular emergencies; Centralisation; GEMS; Ground emergency medical service; HEMS; Helicopter emergency medical service; Interfacility transfers; Myocardial infarction; Stroke; rAAA.
© 2021. The Author(s).
Conflict of interest statement
We declare no competing interests.
Figures
References
-
- Vonlanthen R, Lodge P, Barkun JS, Farges O, Rogiers X, Soreide K, et al. Toward a consensus on centralization in surgery. Ann Surg. 2018;268. - PubMed
-
- Güller U, Warschkow R, Ackermann C, Schmied B, Cerny T, Ess S. Lower hospital volume is associated with higher mortality after oesophageal, gastric, pancreatic and rectal cancer resection. Swiss Med Week. 2017;147. - PubMed
-
- Scali ST, Beck A, Sedrakyan A, Mao J, Behrendt C-A, Boyle JR, et al. Editor’s choice – optimal threshold for the volume–outcome relationship after open AAA repair in the endovascular era: analysis of the international consortium of vascular registries. Eur J Vasc Endovasc Surg. 2021;61. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
