

Clinical characteristics and risk factors associated with mortality in patients with severe community-acquired pneumonia and type 2 diabetes mellitus
- PMID: 34876193
- PMCID: PMC8650350
- DOI: 10.1186/s13054-021-03841-w
Clinical characteristics and risk factors associated with mortality in patients with severe community-acquired pneumonia and type 2 diabetes mellitus
Abstract
Background: The present study was performed to investigate the impacts of type 2 diabetes mellitus (T2DM) on severe community-acquired pneumonia (SCAP) and to develop a novel prediction model for mortality in SCAP patients with T2DM.
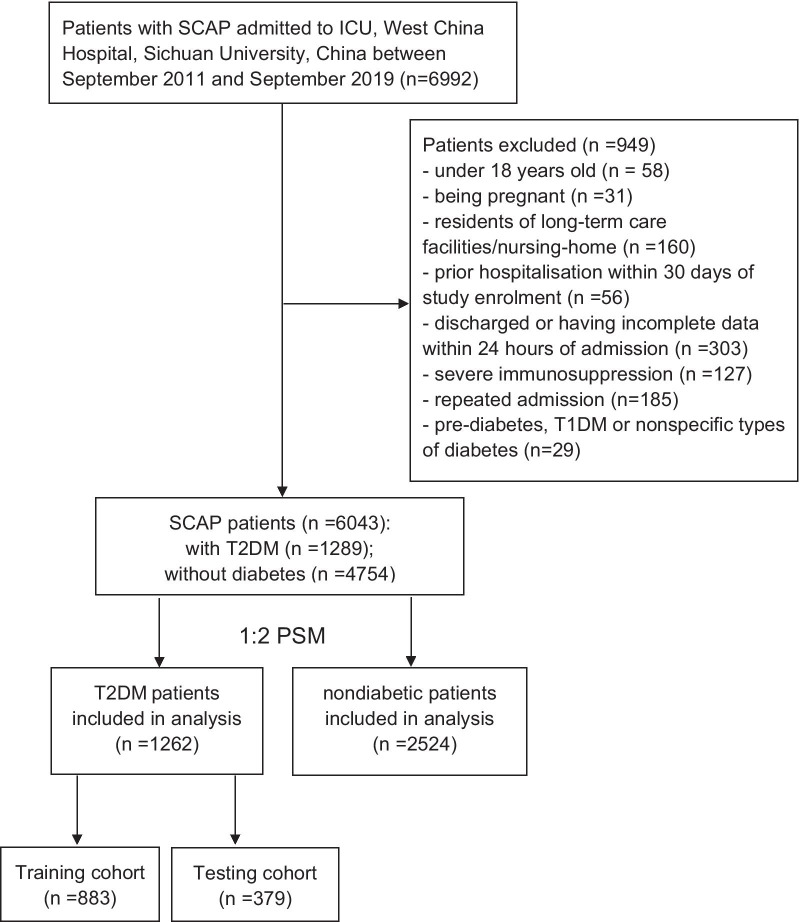
Methods: This was a retrospective observational study conducted in consecutive adult patients with SCAP admitted to the intensive care unit (ICU) of West China Hospital, Sichuan University, China, between September 2011 and September 2019. The primary outcome was hospital mortality. A propensity score matching (PSM) analysis model with a 1:2 ratio was used for the comparisons of clinical characteristics and outcomes between T2DM and nondiabetic patients. The independent risk factors were identified via univariate and then multivariable logistic regression analysis and were then used to establish a nomogram.
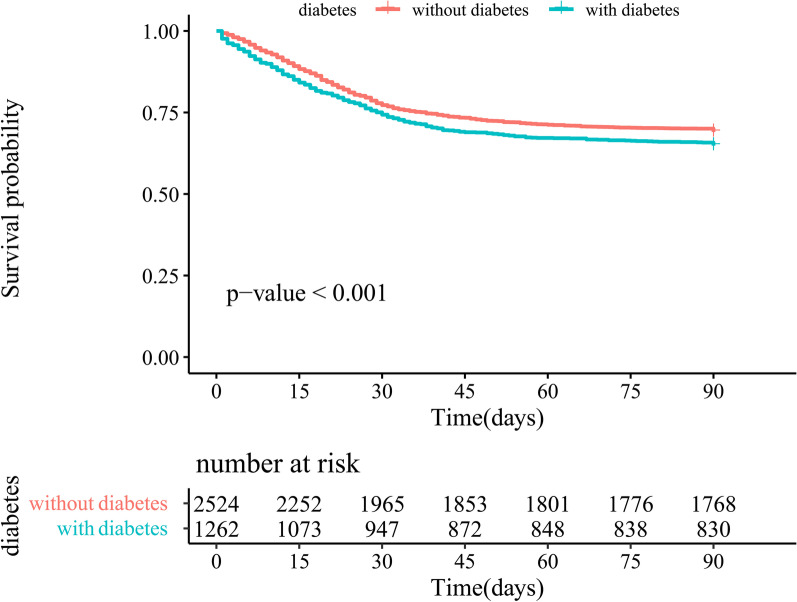
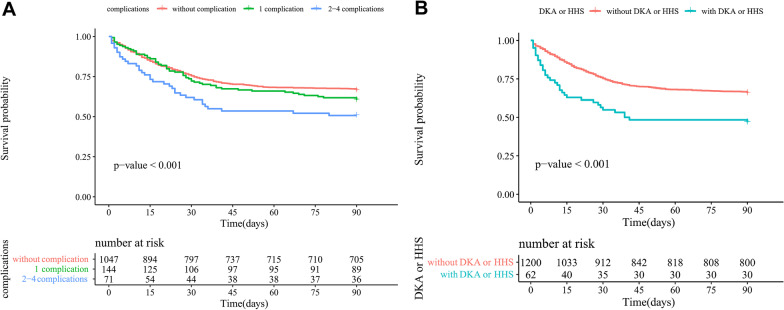
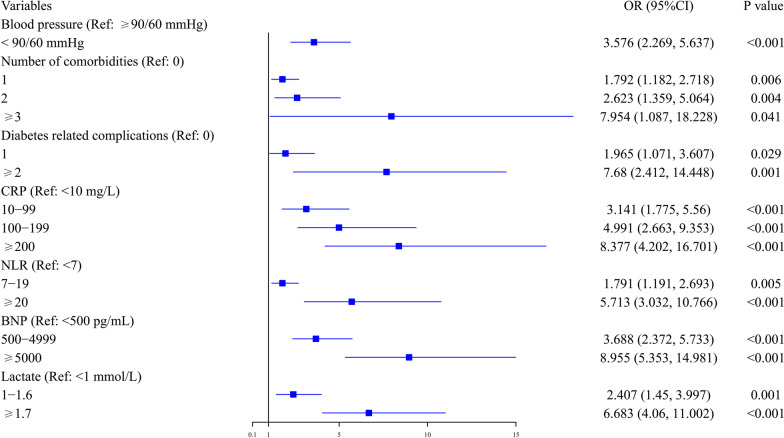
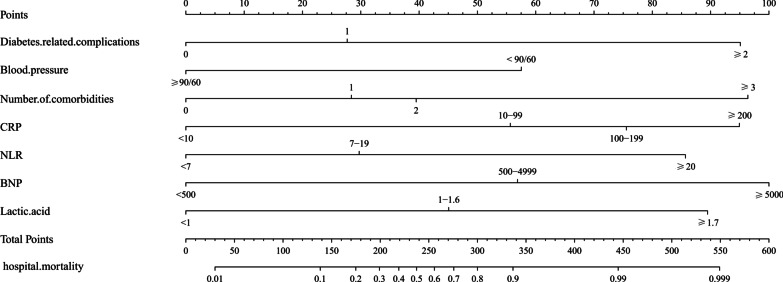
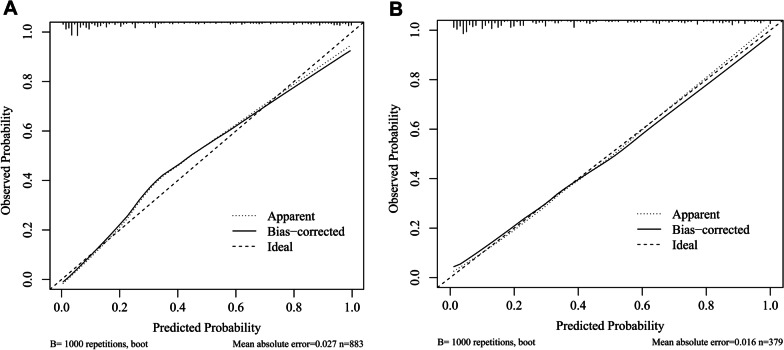
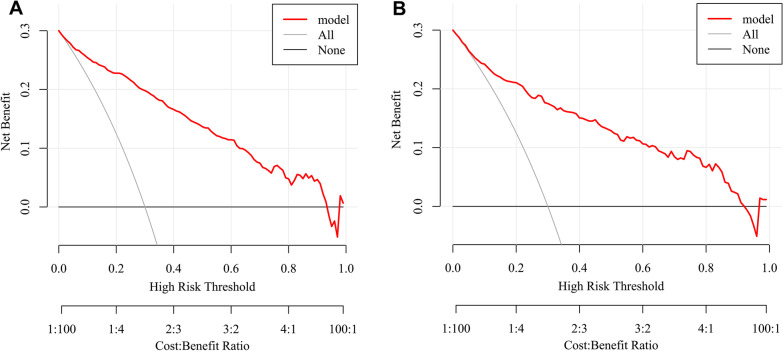
Results: In total, 1262 SCAP patients with T2DM and 2524 matched patients without T2DM were included after PSM. Patients with T2DM had longer ICU length of stay (LOS) (13 vs. 12 days, P = 0.016) and higher 14-day mortality (15% vs. 10.8%, P < 0.001), 30-day mortality (25.7% vs. 22.7%, P = 0.046), ICU mortality (30.8% vs. 26.5%, P = 0.005), and hospital mortality (35.2% vs. 31.0%, P = 0.009) than those without T2DM. In SCAP patients with T2DM, the independent risk factors for hospital mortality were increased numbers of comorbidities and diabetes-related complications; elevated C-reactive protein (CRP), neutrophil to lymphocyte ratio (NLR), brain natriuretic peptide (BNP) and blood lactate; as well as decreased blood pressure on admission. The nomogram had a C index of 0.907 (95% CI: 0.888, 0.927) in the training set and 0.873 (95% CI: 0.836, 0.911) in the testing set, which was superior to the pneumonia severity index (PSI, AUC: 0.809, 95% CI: 0.785, 0.833). The calibration curve and decision curve analysis (DCA) also demonstrated its accuracy and applicability.
Conclusions: SCAP patients with T2DM had worse clinical outcomes than nondiabetic patients. The nomogram has good predictive performance for hospital mortality and might be generally applied after more external validations.
Keywords: Clinical characteristics; Nomogram; Risk factors; Severe community-acquired pneumonia; Type 2 diabetes mellitus.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019;200(7):e45–e67. doi: 10.1164/rccm.201908-1581ST. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
