

Does changing healthcare use signal opportunities for earlier detection of cancer? A review of studies using information from electronic patient records
- PMID: 34876377
- PMCID: PMC8785122
- DOI: 10.1016/j.canep.2021.102072
Does changing healthcare use signal opportunities for earlier detection of cancer? A review of studies using information from electronic patient records
Abstract
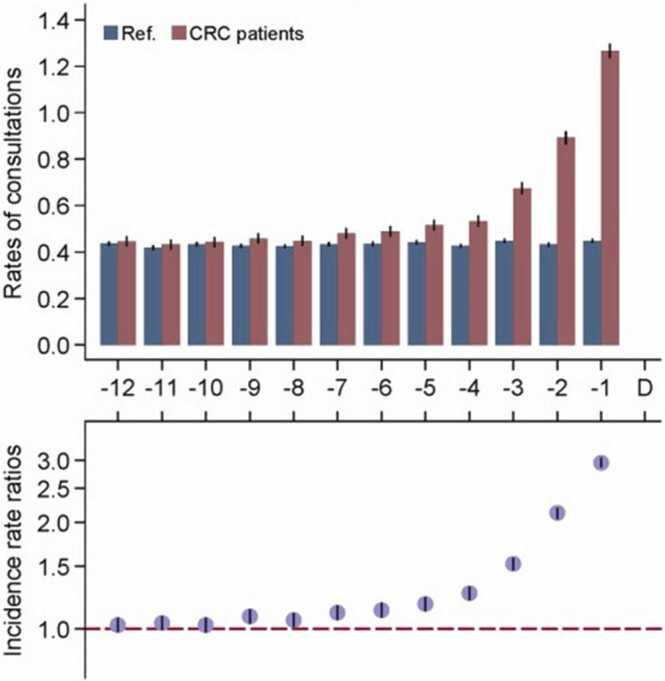
Background: It has been proposed that changes in healthcare use before cancer diagnosis could signal opportunities for quicker detection, but systematic appreciation of such evidence is lacking. We reviewed studies examining pre-diagnostic changes in healthcare utilisation (e.g. rates of GP or hospital consultations, prescriptions or diagnostic tests) among patients subsequently diagnosed with cancer.
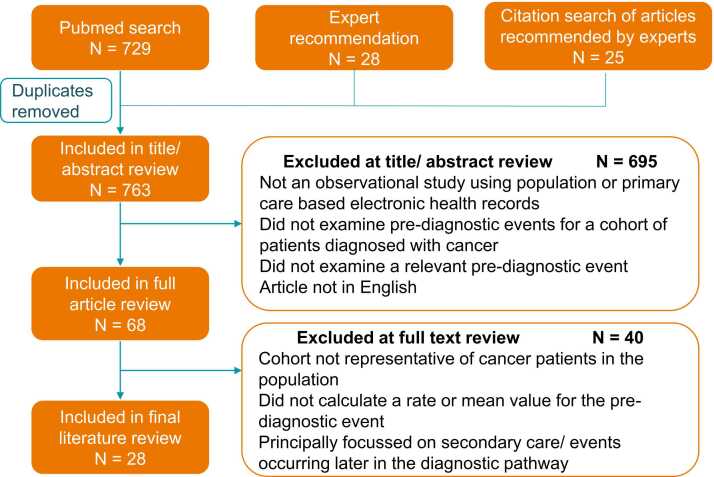
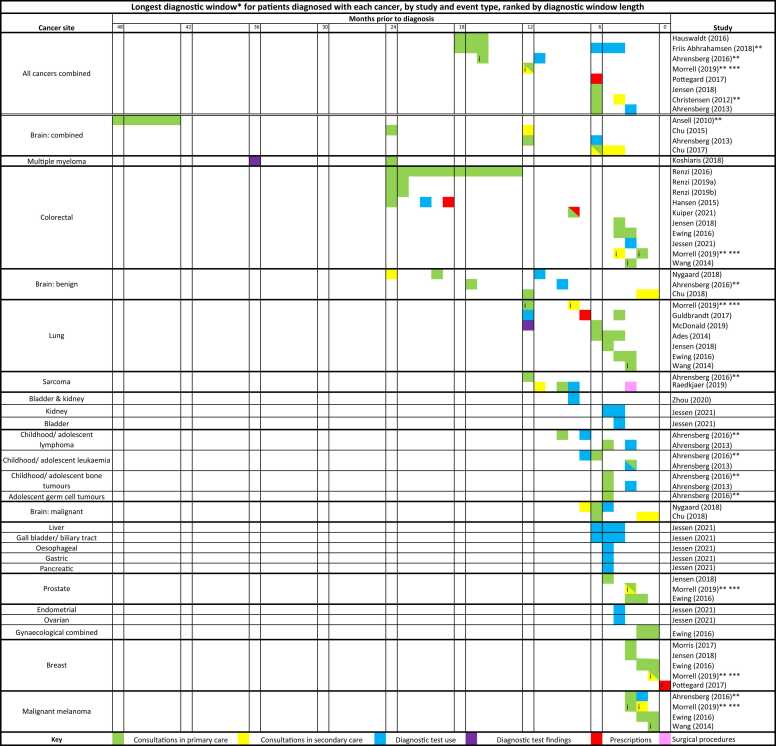
Methods: We identified studies through Pubmed searches complemented by expert elicitation. We extracted information on the earliest time point when diagnosis could have been possible for at least some cancers, together with variation in the length of such 'diagnostic windows' by tumour and patient characteristics.
Results: Across twenty-eight studies, changes in healthcare use were observable at least six months pre-diagnosis for many common cancers, and potentially even earlier for colorectal cancer, multiple myeloma and brain tumours. Early changes were also identified for brain and colon cancer sub-sites.
Conclusion: Changing healthcare utilisation patterns before diagnosis indicate that future improvements in diagnostic technologies or services could help to shorten diagnostic intervals for cancer. There is greatest potential for quicker diagnosis for certain cancer types and patient groups, which can inform priorities for the development of decision support tools.
Keywords: Early detection of cancer[MeSH Term]; Early diagnosis; Health records; Healthcare use; Signs and symptoms[MeSH Term].
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Tørring M.L., Falborg A.Z., Jensen H., Neal R.D., Weller D., Reguilon I., Menon U., Vedsted P., Almberg S.S., Anandan C., Barisic A., Boylan J., Cairnduff V., Donnelly C., Fourkala E.O., Gavin A., Grunfeld E., Hammersley V., Hawryluk B., Kearney T., Kelly J., Knudsen A.K., Lambe M., Law R., Lin Y., Malmberg M., Moore K., Turner D., White V. Advanced‐stage cancer and time to diagnosis: an international cancer benchmarking partnership (ICBP) cross‐sectional study. Eur. J. Cancer Care. 2019;28 doi: 10.1111/ecc.13100. - DOI - PubMed
-
- Neal R.D., Tharmanathan P., France B., Din N.U., Cotton S., Fallon-Ferguson J., Hamilton W., Hendry A., Hendry M., Lewis R., Macleod U., Mitchell E.D., Pickett M., Rai T., Shaw K., Stuart N., Tørring M.L., Wilkinson C., Williams B., Williams N., Emery J. Is increased time to diagnosis and treatment in symptomatic cancer associated with poorer outcomes? systematic review. Br. J. Cancer. 2015;112:S92–S107. doi: 10.1038/bjc.2015.48. - DOI - PMC - PubMed
-
- Tørring M.L., Murchie P., Hamilton W., Vedsted P., Esteva M., Lautrup M., Winget M., Rubin G. Evidence of advanced stage colorectal cancer with longer diagnostic intervals: a pooled analysis of seven primary care cohorts comprising 11 720 patients in five countries. Br. J. Cancer. 2017;117:888–897. doi: 10.1038/bjc.2017.236. - DOI - PMC - PubMed
-
- Mendonca S.C., Abel G.A., Saunders C.L., Wardle J., Lyratzopoulos G. Pre-referral general practitioner consultations and subsequent experience of cancer care: evidence from the english cancer patient experience survey. Eur. J. Cancer Care. 2016;25:478–490. doi: 10.1111/ecc.12353. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
