

Atezolizumab Treatment of Tumors with High Tumor Mutational Burden from MyPathway, a Multicenter, Open-Label, Phase IIa Multiple Basket Study
- PMID: 34876409
- PMCID: PMC9394388
- DOI: 10.1158/2159-8290.CD-21-0450
Atezolizumab Treatment of Tumors with High Tumor Mutational Burden from MyPathway, a Multicenter, Open-Label, Phase IIa Multiple Basket Study
Abstract
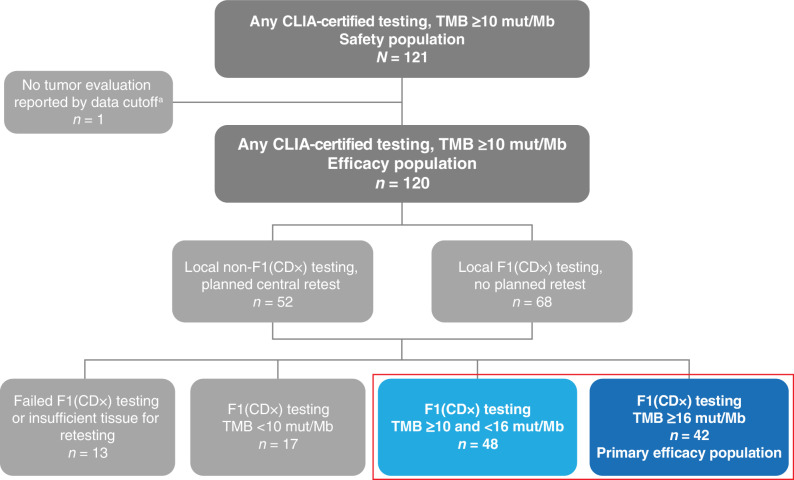
High tumor mutational burden (TMB-H) correlates with improved immunotherapy response. We assessed atezolizumab 1,200 mg every 3 weeks for TMB-H tumors from MyPathway (NCT02091141), a phase IIa multibasket study. One hundred twenty-one patients had advanced solid tumors with TMB ≥10 mut/Mb by any Clinical Laboratory Improvement Amendments (CLIA)-certified assay. The preplanned primary endpoint was objective response rate (ORR) in patients with TMB ≥16 mut/Mb tumors by FoundationOne TMB testing [F1(CDx)]. Patients with F1(CDx) TMB ≥10 and <16 mut/Mb were also evaluated. Ninety patients with 19 tumor types and F1(CDx) TMB ≥10 mut/Mb were efficacy evaluable. In 42 patients with F1(CDx) TMB ≥16 mut/Mb, confirmed ORR was 38.1% [16/42; 95% confidence interval (CI), 23.6-54.4], and disease control rate was 61.9% (26/42; 95% CI, 45.6-76.4) versus 2.1% (1/48; 95% CI, 0.1-11.1) and 22.9% (11/48; 95% CI, 12.0-37.3) for 48 patients with TMB ≥10 and <16 mut/Mb. Responses were observed in nine different tumor types (47%; 9/19).
Significance: Atezolizumab monotherapy had promising, durable clinical activity across a variety of advanced solid tumor types in patients with TMB ≥16 mut/Mb tumors lacking other suitable treatment options and who were immunotherapy-naïve at enrollment, regardless of microsatellite instability status. Limited activity was observed in tumors with TMB ≥10 and <16 mut/Mb. See related commentary by Maron and Klempner, p. 602. This article is highlighted in the In This Issue feature, p. 587.
©2021 The Authors; Published by the American Association for Cancer Research.
Figures



Comment in
-
Are You a TMBeliever? Mutations and Atezolizumab Response in Solid Tumors.Cancer Discov. 2022 Mar 1;12(3):602-603. doi: 10.1158/2159-8290.CD-21-1642. Cancer Discov. 2022. PMID: 35257152
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
