

Multifactorial falls prevention programme compared with usual care in UK care homes for older people: multicentre cluster randomised controlled trial with economic evaluation
- PMID: 34876412
- PMCID: PMC8649897
- DOI: 10.1136/bmj-2021-066991
Multifactorial falls prevention programme compared with usual care in UK care homes for older people: multicentre cluster randomised controlled trial with economic evaluation
Abstract
Objectives: To determine the clinical and cost effectiveness of a multifactorial fall prevention programme compared with usual care in long term care homes.
Design: Multicentre, parallel, cluster randomised controlled trial.
Setting: Long term care homes in the UK, registered to care for older people or those with dementia.
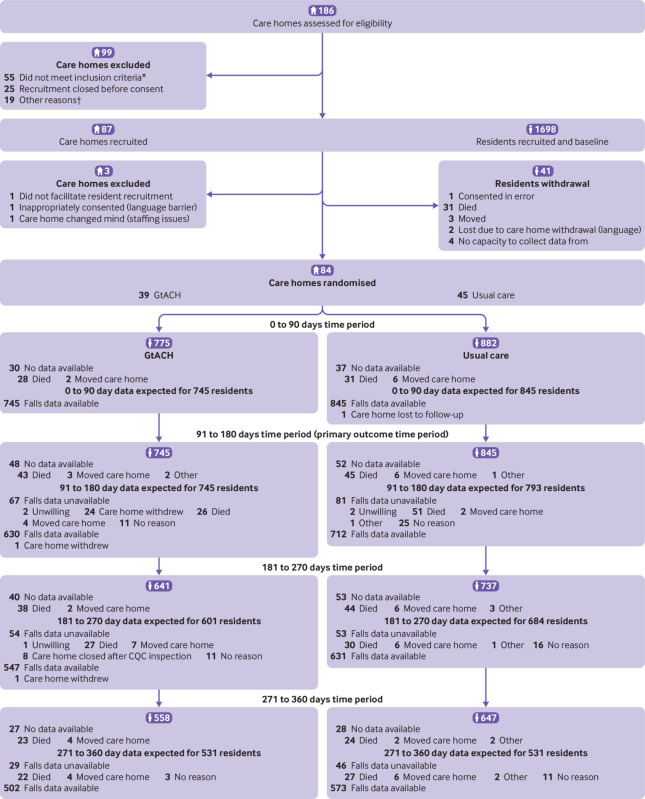
Participants: 1657 consenting residents and 84 care homes. 39 were randomised to the intervention group and 45 were randomised to usual care.
Interventions: Guide to Action for Care Homes (GtACH): a multifactorial fall prevention programme or usual care.
Main outcome measures: Primary outcome measure was fall rate at 91-180 days after randomisation. The economic evaluation measured health related quality of life using quality adjusted life years (QALYs) derived from the five domain five level version of the EuroQoL index (EQ-5D-5L) or proxy version (EQ-5D-5L-P) and the Dementia Quality of Life utility measure (DEMQOL-U), which were self-completed by competent residents and by a care home staff member proxy (DEMQOL-P-U) for all residents (in case the ability to complete changed during the study) until 12 months after randomisation. Secondary outcome measures were falls at 1-90, 181-270, and 271-360 days after randomisation, Barthel index score, and the Physical Activity Measure-Residential Care Homes (PAM-RC) score at 91, 180, 270, and 360 days after randomisation.
Results: Mean age of residents was 85 years. 32% were men. GtACH training was delivered to 1051/1480 staff (71%). Primary outcome data were available for 630 participants in the GtACH group and 712 in the usual care group. The unadjusted incidence rate ratio for falls between 91 and 180 days was 0.57 (95% confidence interval 0.45 to 0.71, P<0.001) in favour of the GtACH programme (GtACH: six falls/1000 residents v usual care: 10 falls/1000). Barthel activities of daily living indices and PAM-RC scores were similar between groups at all time points. The incremental cost was £108 (95% confidence interval -£271.06 to 487.58), incremental QALYs gained for EQ-5D-5L-P was 0.024 (95% confidence interval 0.004 to 0.044) and for DEMQOL-P-U was 0.005 (-0.019 to 0.03). The incremental costs per EQ-5D-5L-P and DEMQOL-P-U based QALY were £4544 and £20 889, respectively.
Conclusions: The GtACH programme was associated with a reduction in fall rate and cost effectiveness, without a decrease in activity or increase in dependency.
Trial registration: ISRCTN34353836.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: funding from the National Institute for Health Research; no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
A multidomain decision support tool to prevent falls in older people: the FinCH cluster RCT.Health Technol Assess. 2022 Jan;26(9):1-136. doi: 10.3310/CWIB0236. Health Technol Assess. 2022. PMID: 35125131 Free PMC article. Clinical Trial.
-
Fall prevention interventions in primary care to reduce fractures and falls in people aged 70 years and over: the PreFIT three-arm cluster RCT.Health Technol Assess. 2021 May;25(34):1-114. doi: 10.3310/hta25340. Health Technol Assess. 2021. PMID: 34075875 Free PMC article. Clinical Trial.
-
Exercise for depression in care home residents: a randomised controlled trial with cost-effectiveness analysis (OPERA).Health Technol Assess. 2013 May;17(18):1-281. doi: 10.3310/hta17180. Health Technol Assess. 2013. PMID: 23632142 Free PMC article. Clinical Trial.
-
Shock-absorbing flooring for fall-related injury prevention in older adults and staff in hospitals and care homes: the SAFEST systematic review.Health Technol Assess. 2022 Jan;26(5):1-196. doi: 10.3310/ZOWL2323. Health Technol Assess. 2022. PMID: 35089119
-
Efficacy and Generalizability of Falls Prevention Interventions in Nursing Homes: A Systematic Review and Meta-analysis.J Am Med Dir Assoc. 2020 Aug;21(8):1024-1035.e4. doi: 10.1016/j.jamda.2019.11.012. Epub 2020 Jan 23. J Am Med Dir Assoc. 2020. PMID: 31982358
Cited by
-
Health care for older adults in Europe: how has it evolved and what are the challenges?Age Ageing. 2022 Dec 5;51(12):afac287. doi: 10.1093/ageing/afac287. Age Ageing. 2022. PMID: 36529998 Free PMC article.
-
FallFitness exercise program provided using the train-the-trainer approach for community-dwelling older adults: a randomized controlled trial.BMC Geriatr. 2024 Nov 30;24(1):983. doi: 10.1186/s12877-024-05575-0. BMC Geriatr. 2024. PMID: 39616365 Free PMC article. Clinical Trial.
-
Predicting future fallers in Parkinson's disease using kinematic data over a period of 5 years.NPJ Digit Med. 2024 Dec 5;7(1):345. doi: 10.1038/s41746-024-01311-5. NPJ Digit Med. 2024. PMID: 39638907 Free PMC article.
-
System-level interventions for fall risk assessment, fall prevention and fall injury prevention in long-term care facilities: a scoping review.Inj Prev. 2024 Oct 30:ip-2024-045386. doi: 10.1136/ip-2024-045386. Online ahead of print. Inj Prev. 2024. PMID: 39477532
-
Trauma recidivism in England and Wales: an epidemiological study.Trauma Surg Acute Care Open. 2025 Jul 15;10(3):e001669. doi: 10.1136/tsaco-2024-001669. eCollection 2025. Trauma Surg Acute Care Open. 2025. PMID: 40673041 Free PMC article.
References
-
- Public Health England. Falls: Applying All Our Health. www.gov.uk/government/publications/falls-applying-all-our-health/falls-a...
-
- Laing W. Care homes for Older People market analysis and projections. 2017. www.laingbuissonevents.com/wp-content/uploads/2017/05/William-COP.pdf
-
- Inspectorate. TC. Managing Falls and Fractures in Care Homes for Older People. 2016. www.careinspectorate.com/images/documents/2737/2016/Falls-and-fractures-...
-
- Oliver D. Preventing falls and falls-injuries in hospitals and long-term care facilities. Rev Clin Gerontol 2007;17:75-91 10.1017/S0959259808002451 . - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous