

Association of persistent acute kidney injury and renal recovery with mortality in hospitalised patients
- PMID: 34876451
- PMCID: PMC8655552
- DOI: 10.1136/bmjhci-2021-100458
Association of persistent acute kidney injury and renal recovery with mortality in hospitalised patients
Abstract
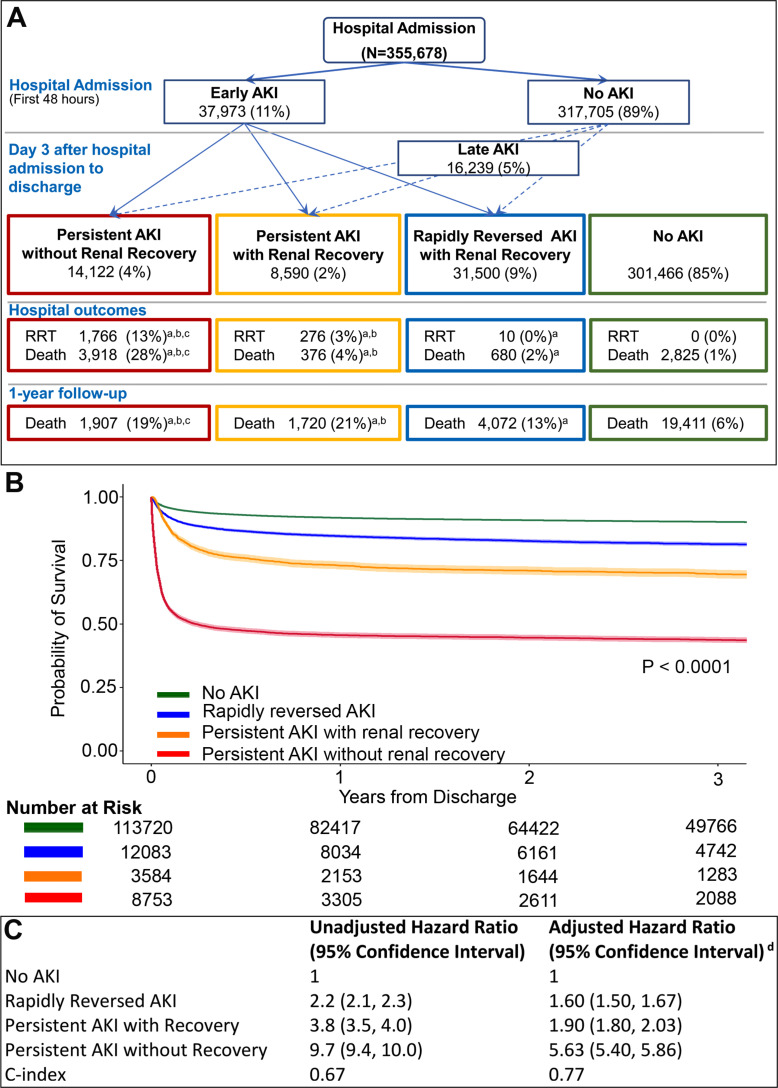
Objectives: Acute kidney injury (AKI) affects up to one-quarter of hospitalised patients and 60% of patients in the intensive care unit (ICU). We aim to understand the baseline characteristics of patients who will develop distinct AKI trajectories, determine the impact of persistent AKI and renal non-recovery on clinical outcomes, resource use, and assess the relative importance of AKI severity, duration and recovery on survival.
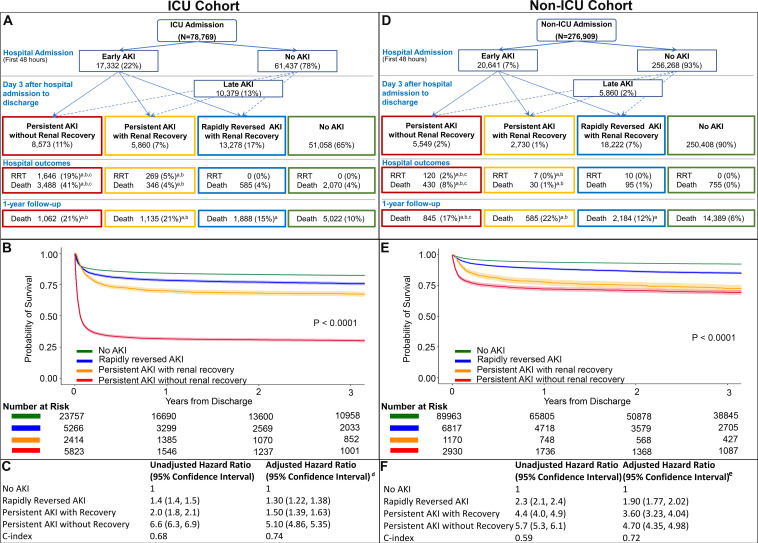
Methods: In this retrospective, longitudinal cohort study, 156 699 patients admitted to a quaternary care hospital between January 2012 and August 2019 were staged and classified (no AKI, rapidly reversed AKI, persistent AKI with and without renal recovery). Clinical outcomes, resource use and short-term and long-term survival adjusting for AKI severity were compared among AKI trajectories in all cohort and subcohorts with and without ICU admission.
Results: Fifty-eight per cent (31 500/54 212) had AKI that rapidly reversed within 48 hours; among patients with persistent AKI, two-thirds (14 122/22 712) did not have renal recovery by discharge. One-year mortality was significantly higher among patients with persistent AKI (35%, 7856/22 712) than patients with rapidly reversed AKI (15%, 4714/31 500) and no AKI (7%, 22 117/301 466). Persistent AKI without renal recovery was associated with approximately fivefold increased hazard rates compared with no AKI in all cohort and ICU and non-ICU subcohorts, independent of AKI severity.
Discussion: Among hospitalised, ICU and non-ICU patients, persistent AKI and the absence of renal recovery are associated with reduced long-term survival, independent of AKI severity.
Conclusions: It is essential to identify patients at risk of developing persistent AKI and no renal recovery to guide treatment-related decisions.
Keywords: critical care outcomes; data interpretation; informatics; statistical.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources