

Early identification of disease progression in ALK-rearranged lung cancer using circulating tumor DNA analysis
- PMID: 34876698
- PMCID: PMC8651695
- DOI: 10.1038/s41698-021-00239-3
Early identification of disease progression in ALK-rearranged lung cancer using circulating tumor DNA analysis
Abstract
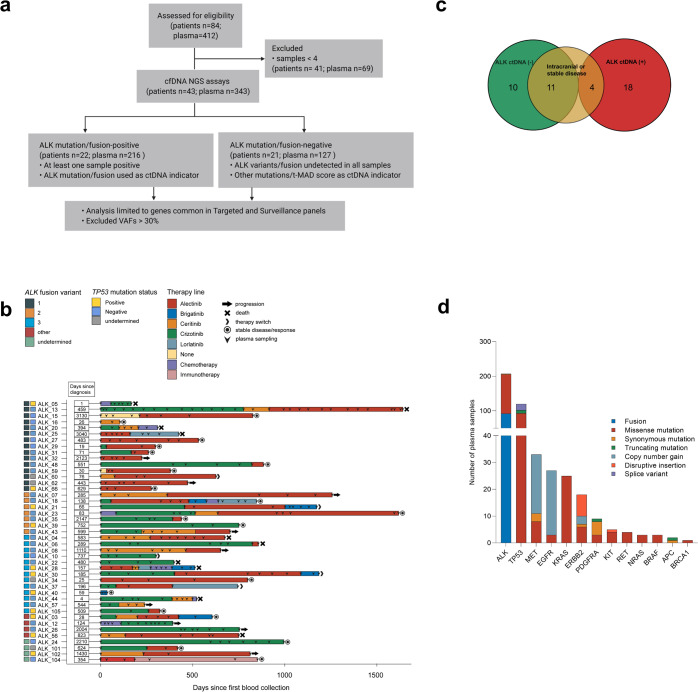
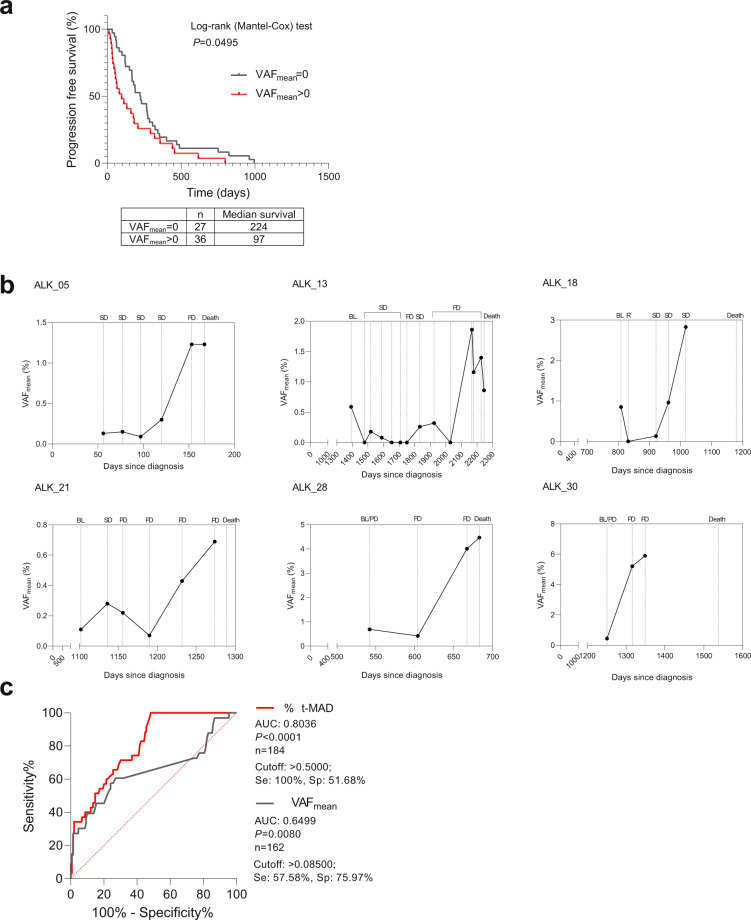
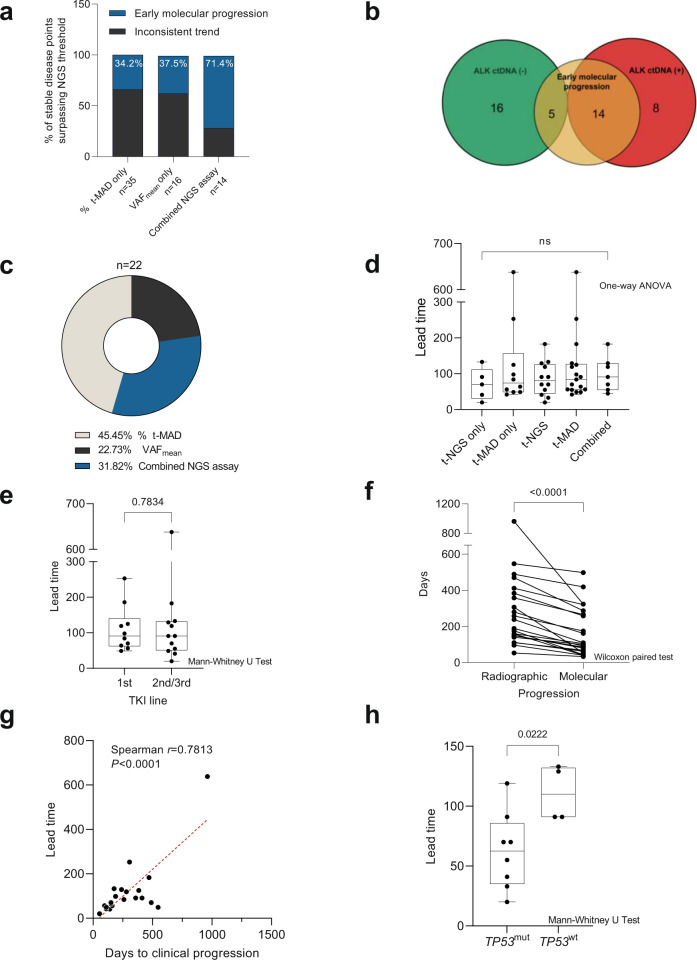
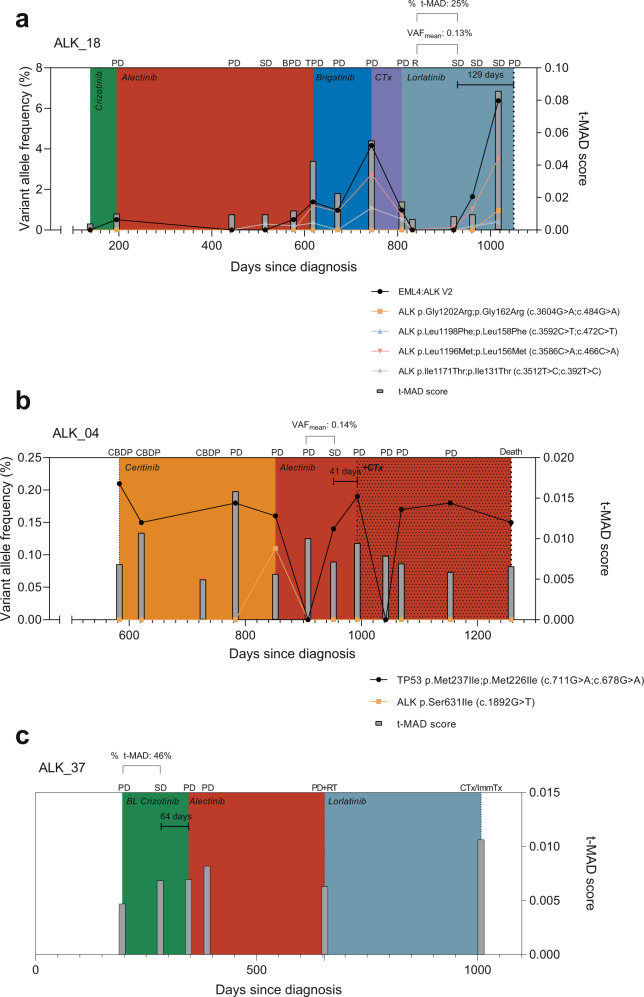
Targeted kinase inhibitors improve the prognosis of lung cancer patients with ALK alterations (ALK+). However, due to the emergence of acquired resistance and varied clinical trajectories, early detection of disease progression is warranted to guide patient management and therapy decisions. We utilized 343 longitudinal plasma DNA samples from 43 ALK+ NSCLC patients receiving ALK-directed therapies to determine molecular progression based on matched panel-based targeted next-generation sequencing (tNGS), and shallow whole-genome sequencing (sWGS). ALK-related alterations were detected in 22 out of 43 (51%) patients. Among 343 longitudinal plasma samples analyzed, 174 (51%) were ctDNA-positive. ALK variant and fusion kinetics generally reflected the disease course. Evidence for early molecular progression was observed in 19 patients (44%). Detection of ctDNA at therapy baseline indicated shorter times to progression compared to cases without mutations at baseline. In patients who succumbed to the disease, ctDNA levels were highly elevated towards the end of life. Our results demonstrate the potential utility of these NGS assays in the clinical management of ALK+ NSCLC.
© 2021. The Author(s).
Conflict of interest statement
P.C. reports research funding from AstraZeneca, Novartis, Roche, and Takeda as well as advisory board and/or lecture fees from Boehringer Ingelheim, Chugai, Lilly, Pfizer, and Takeda, outside the submitted work. M.A.S. reports personal fees from the German Canter for Lung Research (DZL), outside the submitted work. S.D. reports speaker’s honoraria from Roche and research funding from Takeda, outside the submitted work. M.R. reports personal fees from Amgen, AstraZeneca, BMS, Boehringer Ingelheim, Lilly, Merck, MSD, Novartis, Pfizer, Roche, and Samsung, outside the submitted work. M.T. reports advisory board honoraria from Novartis, Lilly, BMS, MSD, Roche, Celgene, Takeda, AbbVie, Boehringer, speaker’s honoraria from Lilly, MSD, Takeda, research funding from AstraZeneca, BMS, Celgene, Novartis, Roche and travel grants from BMS, MSD, Novartis, Boehringer, outside the submitted work. A.S. reports advisory board honoraria from BMS, Bayer, AstraZeneca, Thermo Fisher, Novartis, Seattle Genomics speaker’s honoraria from BMS, Bayer, Illumina, AstraZeneca, Novartis, Thermo Fisher, MSD, Roche, as well as research funding from Chugai, Bayer and BMS, outside the submitted work. H.S. reports grants from Roche Sequencing Solutions, during the conduct of the study, and personal fees from Roche, outside the submitted work. The remaining authors declare no competing interests.
Figures
References
-
- Solomon BJ, et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 2014;371:2167–2177. - PubMed
-
- Kim DW, et al. Brigatinib in patients with crizotinib-refractory anaplastic lymphoma kinase-positive non-small-cell lung cancer: a randomized, multicenter phase II trial. J. Clin. Oncol. 2017;35:2490–2498. - PubMed
LinkOut - more resources
Full Text Sources
