

Nd:YAG Capsulotomy Rates with Two Multifocal Intraocular Lenses
- PMID: 34876835
- PMCID: PMC8643175
- DOI: 10.2147/IJGM.S342039
Nd:YAG Capsulotomy Rates with Two Multifocal Intraocular Lenses
Abstract
Purpose: To investigate the incidence of Nd:YAG capsulotomy after implantation of two types of multifocal intraocular lenses (MIOLs).
Methods: This retrospective analysis included patients who had undergone cataract extraction and implanted diffractive MIOL (Acri. LISA tri 839M) or asymmetric refractive MIOL (SBL-3) from May 2016 to September 2018. They were followed up for at least 3 years. During the follow-up period, the relevant data of patients were kept by special person in the hospital. The rates of Nd:YAG capsulotomy and the Kaplan-Meier survival curve were used to analyze the two groups.
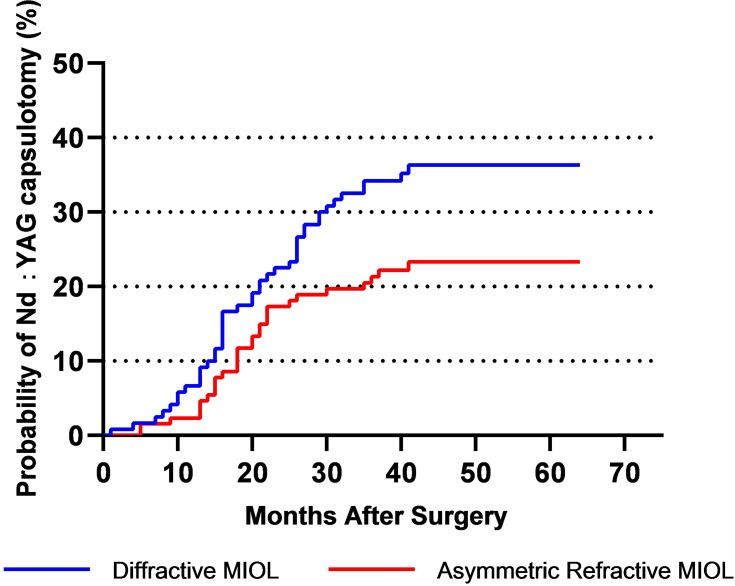
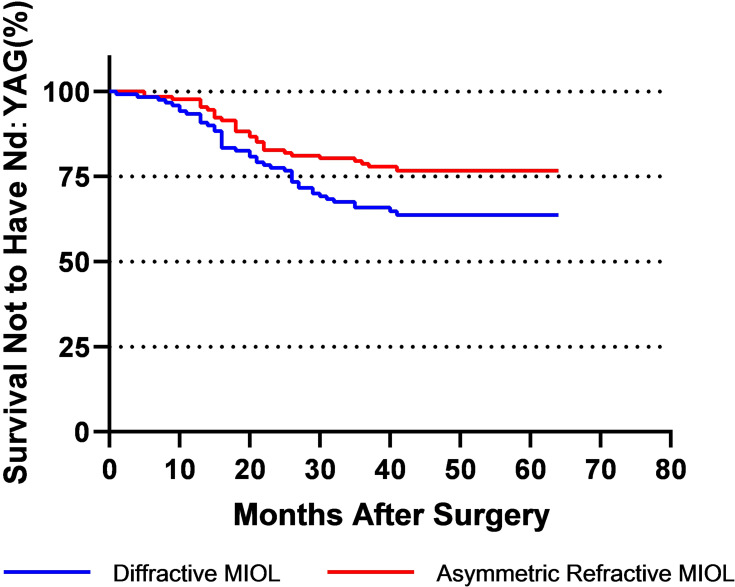
Results: The Asymmetric Refractive MIOL group was comprised of 98 patients (121 eyes), while the Diffractive MIOL group was comprised of 99 patients (120 eyes). There were no significant differences in age, sex, or IOL power between the two groups. The Nd:YAG rate of the asymmetric refractive MIOL group and the diffractive MIOL group was 3.3% and 7.5% respectively (P = 0.15) in the first year, 14.88% and 22.5% respectively (P = 0.129) in the second year, and 21.49% and 34.17% respectively (P = 0.028) in the third year. In the first 7 months of follow-up, the two groups showed the same performance in the Nd:YAG rate. After that, there was a difference between the two groups, and the difference gradually increased. Until the 27th month of follow-up, the difference was significant (P < 0.05). What is more, there were significant differences in survival (without Nd:YAG capsulotomy)/failure (with Nd:YAG capsulotomy) functions (P = 0.0035).
Conclusion: The incidence of Nd:YAG laser capsulotomy in patients with diffractive MIOLs was higher than that in patients with asymmetric refractive MIOLs.
Keywords: Nd:YAG capsulotomy rates; asymmetric refractive MIOL; diffractive MIOL; posterior capsular opacification.
© 2021 Bai et al.
Conflict of interest statement
All authors report no conflicts of interest relevant to this article.
Figures
References
LinkOut - more resources
Full Text Sources
