

The Potential of Visceral Adipose Tissue in Distinguishing Clear Cell Renal Cell Carcinoma from Renal Angiomyolipoma with Minimal Fat
- PMID: 34876853
- PMCID: PMC8643137
- DOI: 10.2147/CMAR.S336920
The Potential of Visceral Adipose Tissue in Distinguishing Clear Cell Renal Cell Carcinoma from Renal Angiomyolipoma with Minimal Fat
Abstract
Purpose: To overcome the challenge of preoperative differentiation between clear cell renal cell carcinoma (ccRCC) and renal angiomyolipoma with minimal fat (RMFAML), we evaluated the potential of visceral adipose tissue (VAT) in distinguishing RMFAML from ccRCC.
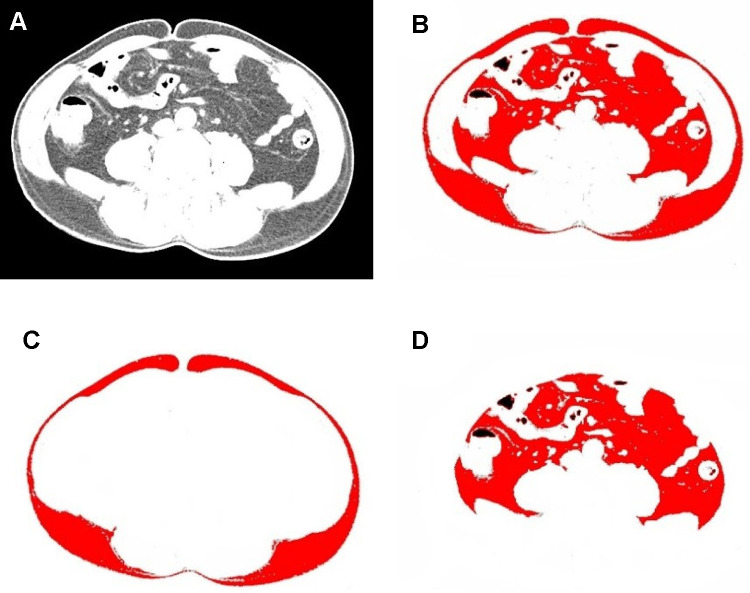
Patients and methods: Patients (191) were divided into ccRCC and RMFAML groups according to postoperative pathology. Umbilical horizontal computed tomography (CT) images were used for visceral fat area (VFA), subcutaneous fat area (SFA) and total fat area (TFA) measurements. Logistic regression was used to identify risk factors for ccRCC. Areas under the receiver operating characteristic (ROC) curve (AUCs) were compared to identify the most valuable indicator for identifying ccRCC and RMFAML.
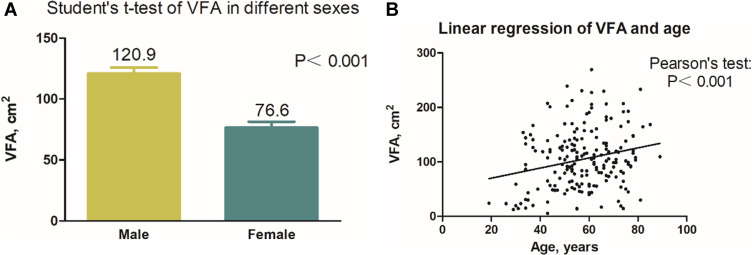
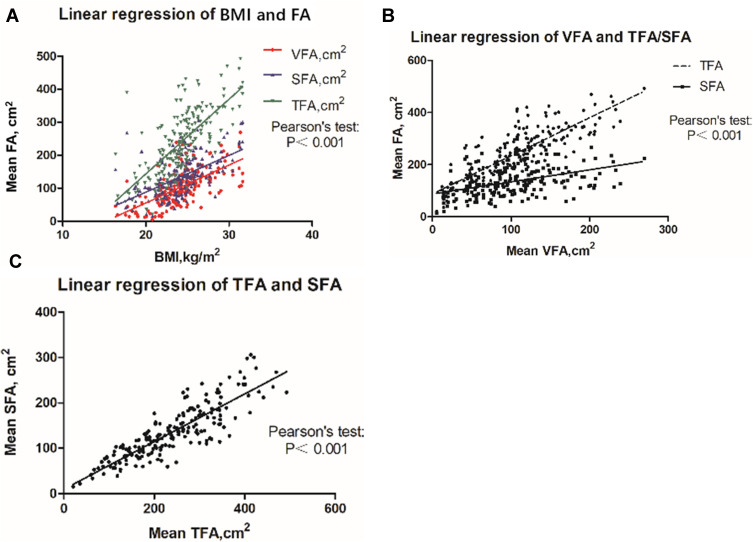
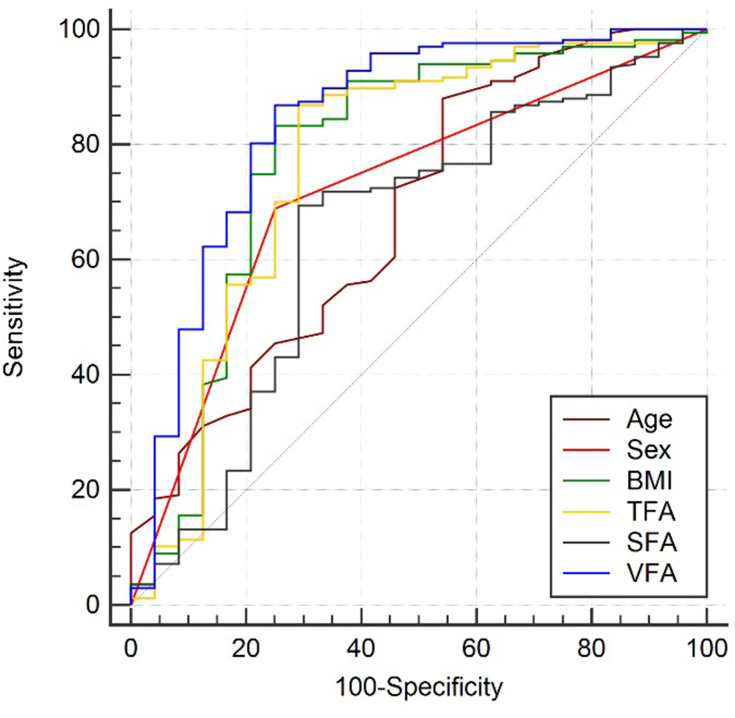
Results: In total, 166 patients had ccRCC, and 25 had RMFAML. ccRCC and RMFAML patients showed significant differences in age (P<0.001), sex (P<0.001), hypertension (P=0.027), BMI (P<0.001), SFA (P=0.046), VFA (P<0.001) and TFA (P<0.001). According to multiple logistic regression analysis, male sex [4.311 (1.469~12.653), p=0.008]; older age [1.047 (1.008~1.088), p=0.017]; and higher BMI [1.305 (1.088~1.566), p=0.004], SFA [1.013 (1.003~1.023), p=0.008], VFA [1.026 (1.012~1.041), p<0.001] and TFA [1.011 (1.005~1.017), p=0.001] were associated with ccRCC. The AUCs of sex (male), age, BMI, TFA, VFA, and SFA were 0.726, 0.687, 0.783, 0.769, 0.840, and 0.645, respectively. The VFA cut-off value was 69.99 cm2. The sensitivity and specificity of higher VFA (≥69.99 cm2) for ccRCC diagnosis were 79.52% and 80.00%, respectively.
Conclusion: In differentiating ccRCC from RMFAML, male sex, older age, and higher BMI, TFA, SFA, and VFA are risk factors for ccRCC. VFA is the most effective indicator for identifying ccRCC.
Keywords: body mass index; clear cell renal cell carcinoma; obesity-related index; renal angiomyolipoma with minimal fat; visceral adipose tissue; visceral fat area.
© 2021 Liu et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Can Gender-Specific Renal and Visceral Fat Be Evaluated by CT Predict Fuhrman Nuclear Classification of Clear Cell Renal Cell Carcinoma?Curr Med Imaging. 2024;20:e15734056295913. doi: 10.2174/0115734056295913240514020603. Curr Med Imaging. 2024. PMID: 38798222
-
Visceral adiposity and inflammatory bowel disease.Int J Colorectal Dis. 2021 Nov;36(11):2305-2319. doi: 10.1007/s00384-021-03968-w. Epub 2021 Jun 9. Int J Colorectal Dis. 2021. PMID: 34104989 Review.
-
The value of sex-specific abdominal visceral fat as measured via CT as a predictor of clear renal cell carcinoma T stage.Adipocyte. 2021 Dec;10(1):285-292. doi: 10.1080/21623945.2021.1924957. Adipocyte. 2021. PMID: 34014795 Free PMC article.
-
Visceral fat accumulation is associated with different pathological subtypes of renal cell carcinoma (RCC): a multicentre study in China.BJU Int. 2014 Oct;114(4):496-502. doi: 10.1111/bju.12592. BJU Int. 2014. PMID: 25383400
-
Diagnostic test accuracy of ADC values for identification of clear cell renal cell carcinoma: systematic review and meta-analysis.Eur Radiol. 2020 Jul;30(7):4023-4038. doi: 10.1007/s00330-020-06740-w. Epub 2020 Mar 6. Eur Radiol. 2020. PMID: 32144458 Free PMC article.
Cited by
-
Nutritional status as a predictive factor for paediatric tuberous sclerosis complex-associated kidney angiomyolipomas: a retrospective analysis.Eur J Pediatr. 2024 Jun;183(6):2563-2570. doi: 10.1007/s00431-024-05520-8. Epub 2024 Mar 14. Eur J Pediatr. 2024. PMID: 38483608 Free PMC article.
-
Spectrum of Presentations and Management Strategies in Renal Angiomyolipoma.J Kidney Cancer VHL. 2022 Jan 28;9(1):42-47. doi: 10.15586/jkcvhl.v9i1.221. eCollection 2022. J Kidney Cancer VHL. 2022. PMID: 35127338 Free PMC article.
-
Stress Reactivity, Susceptibility to Hypertension, and Differential Expression of Genes in Hypertensive Compared to Normotensive Patients.Int J Mol Sci. 2022 Mar 4;23(5):2835. doi: 10.3390/ijms23052835. Int J Mol Sci. 2022. PMID: 35269977 Free PMC article.
-
Comparison of perinephric fat measurements between malignant and benign renal tumours.J Int Med Res. 2022 Sep;50(9):3000605221125086. doi: 10.1177/03000605221125086. J Int Med Res. 2022. PMID: 36172996 Free PMC article.
-
The relationship between renal cell carcinoma pathological types and perirenal fat area.BMC Cancer. 2025 May 8;25(1):841. doi: 10.1186/s12885-025-14164-2. BMC Cancer. 2025. PMID: 40340924 Free PMC article.
References
LinkOut - more resources
Full Text Sources
