

Prognostic Factors and a Nomogram Predicting Survival in Patients with Breast Ductal Carcinoma in situ with Microinvasion: A Population-Based Study
- PMID: 34876856
- PMCID: PMC8643132
- DOI: 10.2147/CLEP.S341422
Prognostic Factors and a Nomogram Predicting Survival in Patients with Breast Ductal Carcinoma in situ with Microinvasion: A Population-Based Study
Abstract
Purpose: Ductal carcinoma in situ with microinvasion (DCISM) can be challenging to balance the risks of overtreatment versus undertreatment. We aim to identify prognostic factors in patients with DCISM and construct a nomogram to predict breast cancer-specific survival (BCSS).
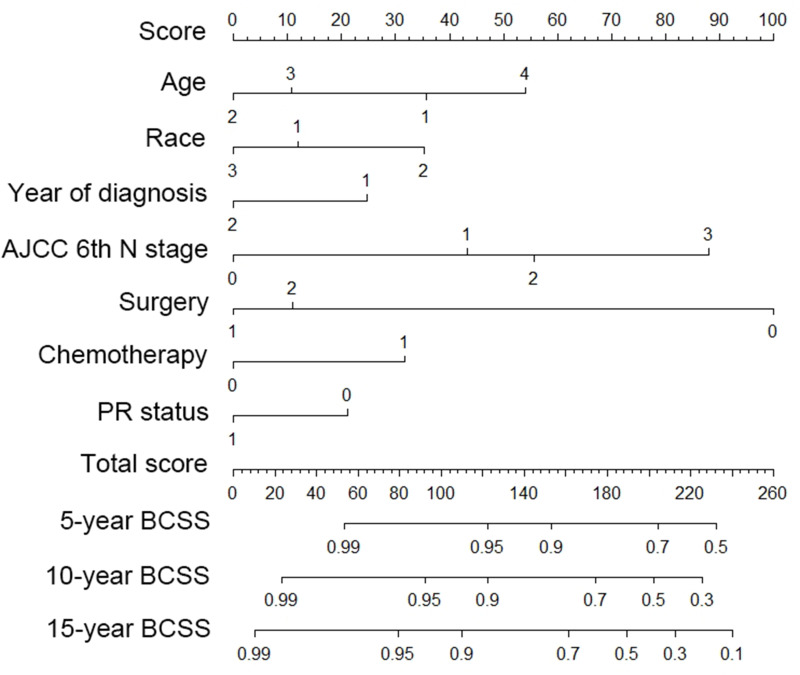
Materials and methods: A retrospective cohort study of women diagnosed with DCISM from 1988 to 2015 who were identified in the Surveillance, Epidemiology and End Results database. Clinical variables and tumor characteristics were evaluated, and Cox proportional-hazards regression was performed. A nomogram was constructed from the multivariate logistic regression to combine all the prognostic factors to predict the prognosis of DCISM patients at 5 years, 10 years, and 15 years.
Results: We identified 5438 total eligible breast cancer patients with a median and max survival time of 78 and 227 months, respectively. Here, patients with poorer survival outcomes were those diagnosed between 1988 and 2001, African-American race, under 40 years of age, higher tumor N stage, progesterone receptor-negative tumor, and received no surgery. The nomogram was constructed by the seven variables and passed the calibration and validation steps. The area under the receiver operating characteristic (ROC) curve (AUC) of both the training set and the validating set (5-year AUC: 0.77 and 0.88, 10-year AUC: 0.75 and 0.73, 15-year AUC: 0.72 and 0.65). Receiving chemotherapy was associated with a better BCSS (hazard ratio, HR=0.45, 95% confidence interval, 95% CI = 0.23-0.89), especially in patients with estrogen receptor (ER) negative, progesterone receptor (PR) negative (HR = 0.35, 95% CI = 0.13-0.97) and ER+PR-/ER-PR+ DCISM (HR = 0.07, 95% CI = 0.01-0.59).
Conclusion: Our current study is the first to construct nomograms of patients with DCISM which could help physicians identify breast cancer patients that more likely to benefit from more intensive treatment and follow-up. Chemotherapy might benefit patients with ER-PR- and ER+PR-/ER-PR+ DCISM.
Keywords: breast cancer; ductal carcinoma in situ; microinvasion; nomogram; survival.
© 2021 Zheng et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures



Similar articles
-
An MRI-Based Radiomics Nomogram to Distinguish Ductal Carcinoma In Situ with Microinvasion From Ductal Carcinoma In Situ of Breast Cancer.Acad Radiol. 2023 Sep;30 Suppl 2:S71-S81. doi: 10.1016/j.acra.2023.03.038. Epub 2023 May 20. Acad Radiol. 2023. PMID: 37211478 Clinical Trial.
-
DCIS with Microinvasion: Is It In Situ or Invasive Disease?Ann Surg Oncol. 2019 Oct;26(10):3124-3132. doi: 10.1245/s10434-019-07556-9. Epub 2019 Jul 24. Ann Surg Oncol. 2019. PMID: 31342393 Free PMC article.
-
The diagnostic value of contrast-enhanced ultrasound combined with clinicopathological features in microinvasive ductal carcinoma in situ.Gland Surg. 2024 Nov 30;13(11):1894-1906. doi: 10.21037/gs-24-211. Epub 2024 Nov 26. Gland Surg. 2024. PMID: 39678406 Free PMC article.
-
Ductal carcinoma in situ with microinvasion: prognostic implications, long-term outcomes, and role of axillary evaluation.Int J Radiat Oncol Biol Phys. 2012 Jan 1;82(1):7-13. doi: 10.1016/j.ijrobp.2010.08.027. Epub 2010 Oct 13. Int J Radiat Oncol Biol Phys. 2012. PMID: 20950955
-
Axillary staging in ductal carcinoma in situ with microinvasion: A meta-analysis.Surg Oncol. 2021 Jun;37:101557. doi: 10.1016/j.suronc.2021.101557. Epub 2021 Mar 31. Surg Oncol. 2021. PMID: 33819852
Cited by
-
Prognostic Markers of Microinvasive Breast Carcinoma: A Systematic Review and Meta-Analysis.Cancers (Basel). 2023 May 31;15(11):3007. doi: 10.3390/cancers15113007. Cancers (Basel). 2023. PMID: 37296968 Free PMC article. Review.
-
Unveiling the Clinical Path of Microinvasive Breast Cancer: A Comparative Study With Tis-T1 Breast Cancer.Cancer Med. 2024 Oct;13(19):e70297. doi: 10.1002/cam4.70297. Cancer Med. 2024. PMID: 39382213 Free PMC article.
-
Clinicopathological characteristics, treatments, and prognosis of breast ductal carcinoma in situ with microinvasion: A narrative review.Chronic Dis Transl Med. 2022 Nov 26;9(1):5-13. doi: 10.1002/cdt3.53. eCollection 2023 Mar. Chronic Dis Transl Med. 2022. PMID: 36926252 Free PMC article. Review.
-
Clinicopathological characteristics and prognosis of microinvasive breast cancer: A population-based analysis.Cancer Med. 2022 Dec;11(23):4501-4512. doi: 10.1002/cam4.4839. Epub 2022 May 22. Cancer Med. 2022. PMID: 35598300 Free PMC article. Clinical Trial.
-
Developing and validating nomograms for predicting the survival in patients with clinical local-advanced gastric cancer.Front Oncol. 2022 Oct 26;12:1039498. doi: 10.3389/fonc.2022.1039498. eCollection 2022. Front Oncol. 2022. PMID: 36387146 Free PMC article.
References
-
- Lakhani SR. Who Classification of Tumours of the Breast. International Agency for Research on Cancer; 2012.
-
- Edge SB, Byrd DR, Carducci MA, et al. AJCC Cancer Staging Manual. 7th ed; Springer, New York 2010.
-
- Hoda S, Chiu A, Prasad M, et al. Are microinvasion and micrometastasis in breast cancer mountains or molehills? Am J Surg. 2000;180:305–308. - PubMed
-
- Adamovich T, Simmons R. Ductal carcinoma in situ with microinvasion. Am J Surg. 2003;186:112–116. - PubMed
-
- Bianchi S, Vezzosi V. Microinvasive carcinoma of the breast. Pathol Oncol Res. 2008;14:105–111. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
