

Switching from omalizumab to mepolizumab therapy improved extra-pulmonary abdominal and cutaneous vasculitis symptoms in a patient with eosinophilic granulomatosis with polyangiitis
- PMID: 34876987
- PMCID: PMC8629745
- DOI: 10.1002/rcr2.878
Switching from omalizumab to mepolizumab therapy improved extra-pulmonary abdominal and cutaneous vasculitis symptoms in a patient with eosinophilic granulomatosis with polyangiitis
Abstract
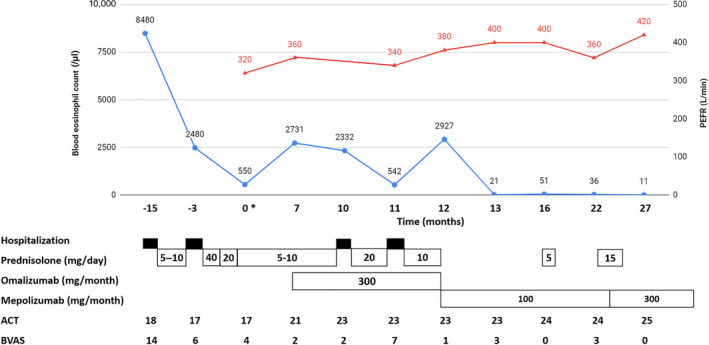
Eosinophilic granulomatosis with polyangiitis (EGPA) is a systemic vasculitis of small-to-medium-sized vessels. Both eosinophilic infiltration and vasculitis are thought to contribute to multi-organ damage. Some biologics have been used to reduce the required dose of corticosteroids in EGPA, but no single agent can ensure a complete control of this disease. Here, we describe a patient with anti-neutrophil cytoplasmic antibodies-negative relapsing EGPA whose asthma control was improved by omalizumab, but she continued to develop flares of abdominal and cutaneous vasculitis symptoms. After switching to mepolizumab therapy, her blood hypereosinophilia and extra-pulmonary symptoms were significantly improved. Moreover, the dose of daily maintenance corticosteroid could be tapered off. The experience from our case suggests that biologics targeting interleukin-5 may be more effective than omalizumab in the management of extra-thoracic manifestations in EGPA.
Keywords: eosinophilic granulomatosis with polyangiitis; extra‐pulmonary; mepolizumab; omalizumab; switching.
© 2021 The Authors. Respirology Case Reports published by John Wiley & Sons Australia, Ltd on behalf of The Asian Pacific Society of Respirology.
Conflict of interest statement
None declared.
Figures

References
-
- Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013;65(1):1–11. - PubMed
-
- Masi AT, Hunder GG, Lie JT, Michel BA, Bloch DA, Arend WP, et al. The American College of Rheumatology 1990 criteria for the classification of Churg‐Strauss syndrome (allergic granulomatosis and angiitis). Arthritis Rheum. 1990;33(8):1094–100. - PubMed
-
- Lanham JG, Elkon KB, Pusey CD, Hughes GR. Systemic vasculitis with asthma and eosinophilia: a clinical approach to the Churg‐Strauss syndrome. Medicine (Baltimore). 1984;63(2):65–81. - PubMed
-
- Comarmond C, Pagnoux C, Khellaf M, Cordier JF, Hamidou M, Viallard JF, et al. Eosinophilic granulomatosis with polyangiitis (Churg‐Strauss): clinical characteristics and long‐term followup of the 383 patients enrolled in the French Vasculitis Study Group cohort. Arthritis Rheum. 2013;65(1):270–81. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
